Ryan B Smithee, Tiffanie M Markus, Elizabeth Soda, Carlos G Grijalva, Wei Xing, Nong Shang, Marie R Griffin, Fernanda C Lessa
{"title":"肺炎住院编码变化与《国际疾病分类》第九版到第十版的过渡相关","authors":"Ryan B Smithee, Tiffanie M Markus, Elizabeth Soda, Carlos G Grijalva, Wei Xing, Nong Shang, Marie R Griffin, Fernanda C Lessa","doi":"10.1177/2333392820939801","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To evaluate the impact of <i>International Classification of Disease</i>, 10th revision, Clinical Modification (<i>ICD-10-CM</i>) implementation on pneumonia hospitalizations rates, which had declined following pneumococcal conjugate vaccine introduction for infants in 2000.</p><p><strong>Methods: </strong>We randomly selected records from a single hospital 1 year before (n = 500) and after (n = 500) October 2015 implementation of <i>ICD-10-CM</i> coding. We used a validated <i>ICD-9-CM</i> algorithm and translation of that algorithm to <i>ICD-10-CM</i> to identify pneumonia hospitalizations pre- and post-implementation, respectively. We recoded <i>ICD-10-CM</i> records to <i>ICD-9-CM</i> and vice versa. We calculated sensitivity and positive predictive value (PPV) of the <i>ICD-10-CM</i> algorithm using <i>ICD-9-CM</i> coding as the reference. We used sensitivity and PPV values to calculate an adjustment factor to apply to <i>ICD-10</i> era rates to enable comparison with <i>ICD-9-CM</i> rates. We reviewed primary diagnoses of charts not meeting the pneumonia definition when recoded.</p><p><strong>Results: </strong>Sensitivity and PPV of the <i>ICD-10-CM</i> algorithm were 94% and 92%, respectively, for young children and 74% and 79% for older adults. The estimated adjustment factor for <i>ICD-10-CM</i> period rates was -2.09% (95% credible region [CR], -7.71% to +3.0%) for children and +6.76% (95% CR, -3.06% to +16.7%) for older adults. We identified a change in coding adult charts that met the <i>ICD-9-CM</i> pneumonia definition that led to recoding in <i>ICD-10-CM</i> as chronic obstructive pulmonary disease (COPD) exacerbation.</p><p><strong>Conclusions: </strong>The <i>ICD-10-CM</i> algorithm derived from a validated <i>ICD-9-CM</i> algorithm should not introduce substantial bias for evaluating pneumonia trends in children. However, changes in coding of pneumonia associated with COPD in adults warrant further study.</p>","PeriodicalId":12951,"journal":{"name":"Health Services Research and Managerial Epidemiology","volume":"7 ","pages":"2333392820939801"},"PeriodicalIF":1.5000,"publicationDate":"2020-07-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1177/2333392820939801","citationCount":"11","resultStr":"{\"title\":\"Pneumonia Hospitalization Coding Changes Associated With Transition From the 9th to 10th Revision of <i>International Classification of Diseases</i>.\",\"authors\":\"Ryan B Smithee, Tiffanie M Markus, Elizabeth Soda, Carlos G Grijalva, Wei Xing, Nong Shang, Marie R Griffin, Fernanda C Lessa\",\"doi\":\"10.1177/2333392820939801\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>To evaluate the impact of <i>International Classification of Disease</i>, 10th revision, Clinical Modification (<i>ICD-10-CM</i>) implementation on pneumonia hospitalizations rates, which had declined following pneumococcal conjugate vaccine introduction for infants in 2000.</p><p><strong>Methods: </strong>We randomly selected records from a single hospital 1 year before (n = 500) and after (n = 500) October 2015 implementation of <i>ICD-10-CM</i> coding. We used a validated <i>ICD-9-CM</i> algorithm and translation of that algorithm to <i>ICD-10-CM</i> to identify pneumonia hospitalizations pre- and post-implementation, respectively. We recoded <i>ICD-10-CM</i> records to <i>ICD-9-CM</i> and vice versa. We calculated sensitivity and positive predictive value (PPV) of the <i>ICD-10-CM</i> algorithm using <i>ICD-9-CM</i> coding as the reference. We used sensitivity and PPV values to calculate an adjustment factor to apply to <i>ICD-10</i> era rates to enable comparison with <i>ICD-9-CM</i> rates. We reviewed primary diagnoses of charts not meeting the pneumonia definition when recoded.</p><p><strong>Results: </strong>Sensitivity and PPV of the <i>ICD-10-CM</i> algorithm were 94% and 92%, respectively, for young children and 74% and 79% for older adults. The estimated adjustment factor for <i>ICD-10-CM</i> period rates was -2.09% (95% credible region [CR], -7.71% to +3.0%) for children and +6.76% (95% CR, -3.06% to +16.7%) for older adults. We identified a change in coding adult charts that met the <i>ICD-9-CM</i> pneumonia definition that led to recoding in <i>ICD-10-CM</i> as chronic obstructive pulmonary disease (COPD) exacerbation.</p><p><strong>Conclusions: </strong>The <i>ICD-10-CM</i> algorithm derived from a validated <i>ICD-9-CM</i> algorithm should not introduce substantial bias for evaluating pneumonia trends in children. However, changes in coding of pneumonia associated with COPD in adults warrant further study.</p>\",\"PeriodicalId\":12951,\"journal\":{\"name\":\"Health Services Research and Managerial Epidemiology\",\"volume\":\"7 \",\"pages\":\"2333392820939801\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2020-07-24\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1177/2333392820939801\",\"citationCount\":\"11\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Health Services Research and Managerial Epidemiology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/2333392820939801\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"HEALTH POLICY & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Health Services Research and Managerial Epidemiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/2333392820939801","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"HEALTH POLICY & SERVICES","Score":null,"Total":0}
Pneumonia Hospitalization Coding Changes Associated With Transition From the 9th to 10th Revision of International Classification of Diseases.
Objectives: To evaluate the impact of International Classification of Disease, 10th revision, Clinical Modification (ICD-10-CM) implementation on pneumonia hospitalizations rates, which had declined following pneumococcal conjugate vaccine introduction for infants in 2000.
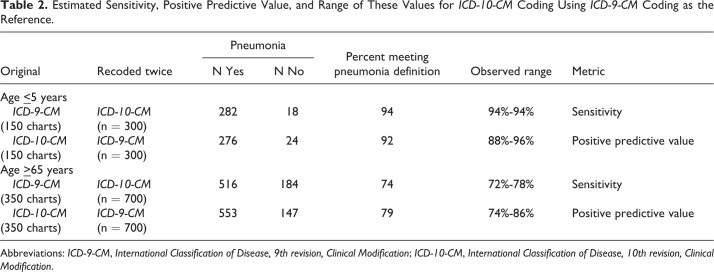
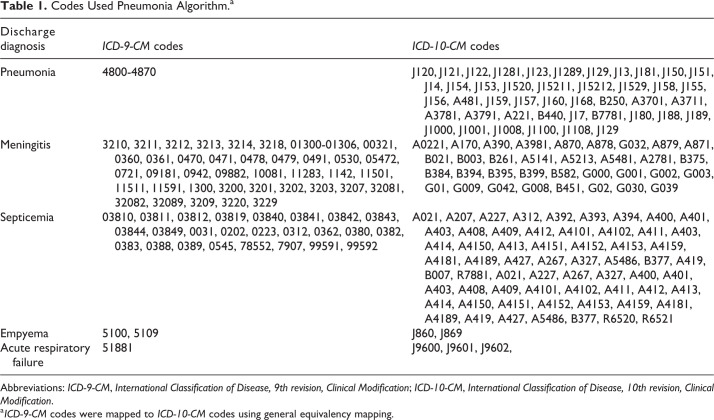
Methods: We randomly selected records from a single hospital 1 year before (n = 500) and after (n = 500) October 2015 implementation of ICD-10-CM coding. We used a validated ICD-9-CM algorithm and translation of that algorithm to ICD-10-CM to identify pneumonia hospitalizations pre- and post-implementation, respectively. We recoded ICD-10-CM records to ICD-9-CM and vice versa. We calculated sensitivity and positive predictive value (PPV) of the ICD-10-CM algorithm using ICD-9-CM coding as the reference. We used sensitivity and PPV values to calculate an adjustment factor to apply to ICD-10 era rates to enable comparison with ICD-9-CM rates. We reviewed primary diagnoses of charts not meeting the pneumonia definition when recoded.
Results: Sensitivity and PPV of the ICD-10-CM algorithm were 94% and 92%, respectively, for young children and 74% and 79% for older adults. The estimated adjustment factor for ICD-10-CM period rates was -2.09% (95% credible region [CR], -7.71% to +3.0%) for children and +6.76% (95% CR, -3.06% to +16.7%) for older adults. We identified a change in coding adult charts that met the ICD-9-CM pneumonia definition that led to recoding in ICD-10-CM as chronic obstructive pulmonary disease (COPD) exacerbation.
Conclusions: The ICD-10-CM algorithm derived from a validated ICD-9-CM algorithm should not introduce substantial bias for evaluating pneumonia trends in children. However, changes in coding of pneumonia associated with COPD in adults warrant further study.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


