Jamie Bloom, David Wyler, Marc C Torjman, Tuan Trinh, Lucy Li, Amy Mehta, Evan Fitchett, David Kastenberg, Michael Mahla, Victor Romo
{"title":"门诊结肠镜检查异丙酚镇静期间爆发抑制的高发生率:从神经监测中获得的经验教训。","authors":"Jamie Bloom, David Wyler, Marc C Torjman, Tuan Trinh, Lucy Li, Amy Mehta, Evan Fitchett, David Kastenberg, Michael Mahla, Victor Romo","doi":"10.1155/2020/7246570","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Although anesthesia providers may plan for moderate sedation, the depth of sedation is rarely quantified. Using processed electroencephalography (EEG) to assess the depth of sedation, this study investigates the incidence of general anesthesia with variable burst suppression in patients receiving propofol for outpatient colonoscopy. The lessons learned from neuromonitoring can then be used to guide institutional best sedation practice.</p><p><strong>Methods: </strong>This was a prospective observational study of 119 outpatients undergoing colonoscopy at Thomas Jefferson University Hospital (TJUH). Propofol was administered by CRNAs under anesthesiologists' supervision. The Patient State Index (PSi™) generated by the Masimo SedLine® Brain Root Function monitor (Masimo Corp., Irvine, CA) was used to assess the depth of sedation. PSi data correlating to general anesthesia with variable burst suppression were confirmed by neuroelectrophysiologists' interpretation of unprocessed EEG.</p><p><strong>Results: </strong>PSi values of <50 consistent with general anesthesia were attained in 118/119 (99.1%) patients. Of these patients, 33 (27.7%) attained PSi values <25 consistent with variable burst suppression. The 118 patients that reached PSi <50 spent a significantly greater percentage (53.1% vs. 42%) of their case at PSi levels <50 compared to PSi levels >50 (<i>p</i>=0.001). Mean total propofol dose was significantly correlated to patient PSi during periods of PSi <25 (<i>R</i>=0.406, <i>p</i>=0.021).</p><p><strong>Conclusion: </strong>Although providers planned for moderate to deep sedation, processed EEG showed patients were under general anesthesia, often with burst suppression. Anesthesiologists and endoscopists may utilize processed EEG to recognize their institutional practice patterns of procedural sedation with propofol and improve upon it.</p>","PeriodicalId":7834,"journal":{"name":"Anesthesiology Research and Practice","volume":"2020 ","pages":"7246570"},"PeriodicalIF":1.6000,"publicationDate":"2020-06-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2020/7246570","citationCount":"7","resultStr":"{\"title\":\"High Incidence of Burst Suppression during Propofol Sedation for Outpatient Colonoscopy: Lessons Learned from Neuromonitoring.\",\"authors\":\"Jamie Bloom, David Wyler, Marc C Torjman, Tuan Trinh, Lucy Li, Amy Mehta, Evan Fitchett, David Kastenberg, Michael Mahla, Victor Romo\",\"doi\":\"10.1155/2020/7246570\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Although anesthesia providers may plan for moderate sedation, the depth of sedation is rarely quantified. Using processed electroencephalography (EEG) to assess the depth of sedation, this study investigates the incidence of general anesthesia with variable burst suppression in patients receiving propofol for outpatient colonoscopy. The lessons learned from neuromonitoring can then be used to guide institutional best sedation practice.</p><p><strong>Methods: </strong>This was a prospective observational study of 119 outpatients undergoing colonoscopy at Thomas Jefferson University Hospital (TJUH). Propofol was administered by CRNAs under anesthesiologists' supervision. The Patient State Index (PSi™) generated by the Masimo SedLine® Brain Root Function monitor (Masimo Corp., Irvine, CA) was used to assess the depth of sedation. PSi data correlating to general anesthesia with variable burst suppression were confirmed by neuroelectrophysiologists' interpretation of unprocessed EEG.</p><p><strong>Results: </strong>PSi values of <50 consistent with general anesthesia were attained in 118/119 (99.1%) patients. Of these patients, 33 (27.7%) attained PSi values <25 consistent with variable burst suppression. The 118 patients that reached PSi <50 spent a significantly greater percentage (53.1% vs. 42%) of their case at PSi levels <50 compared to PSi levels >50 (<i>p</i>=0.001). Mean total propofol dose was significantly correlated to patient PSi during periods of PSi <25 (<i>R</i>=0.406, <i>p</i>=0.021).</p><p><strong>Conclusion: </strong>Although providers planned for moderate to deep sedation, processed EEG showed patients were under general anesthesia, often with burst suppression. Anesthesiologists and endoscopists may utilize processed EEG to recognize their institutional practice patterns of procedural sedation with propofol and improve upon it.</p>\",\"PeriodicalId\":7834,\"journal\":{\"name\":\"Anesthesiology Research and Practice\",\"volume\":\"2020 \",\"pages\":\"7246570\"},\"PeriodicalIF\":1.6000,\"publicationDate\":\"2020-06-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1155/2020/7246570\",\"citationCount\":\"7\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Anesthesiology Research and Practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2020/7246570\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"ANESTHESIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Anesthesiology Research and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2020/7246570","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
High Incidence of Burst Suppression during Propofol Sedation for Outpatient Colonoscopy: Lessons Learned from Neuromonitoring.
Background: Although anesthesia providers may plan for moderate sedation, the depth of sedation is rarely quantified. Using processed electroencephalography (EEG) to assess the depth of sedation, this study investigates the incidence of general anesthesia with variable burst suppression in patients receiving propofol for outpatient colonoscopy. The lessons learned from neuromonitoring can then be used to guide institutional best sedation practice.
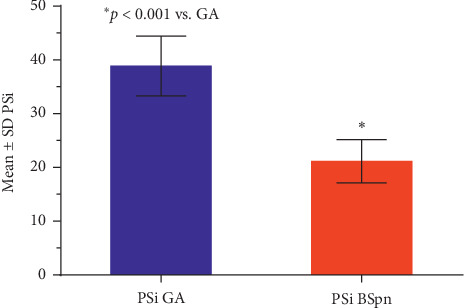
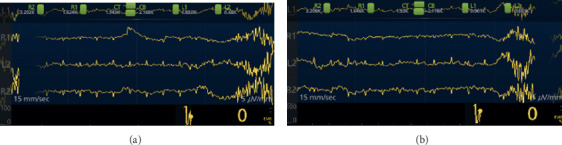
Methods: This was a prospective observational study of 119 outpatients undergoing colonoscopy at Thomas Jefferson University Hospital (TJUH). Propofol was administered by CRNAs under anesthesiologists' supervision. The Patient State Index (PSi™) generated by the Masimo SedLine® Brain Root Function monitor (Masimo Corp., Irvine, CA) was used to assess the depth of sedation. PSi data correlating to general anesthesia with variable burst suppression were confirmed by neuroelectrophysiologists' interpretation of unprocessed EEG.
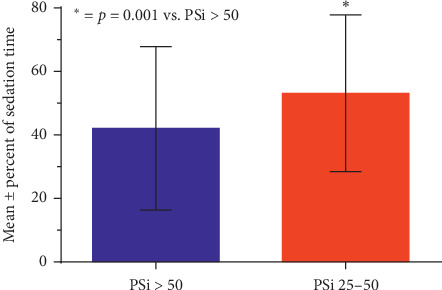
Results: PSi values of <50 consistent with general anesthesia were attained in 118/119 (99.1%) patients. Of these patients, 33 (27.7%) attained PSi values <25 consistent with variable burst suppression. The 118 patients that reached PSi <50 spent a significantly greater percentage (53.1% vs. 42%) of their case at PSi levels <50 compared to PSi levels >50 (p=0.001). Mean total propofol dose was significantly correlated to patient PSi during periods of PSi <25 (R=0.406, p=0.021).
Conclusion: Although providers planned for moderate to deep sedation, processed EEG showed patients were under general anesthesia, often with burst suppression. Anesthesiologists and endoscopists may utilize processed EEG to recognize their institutional practice patterns of procedural sedation with propofol and improve upon it.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


