Mercy Mvundura , Laura Di Giorgio , Chloe Morozoff , Jane Cover , Marguerite Ndour , Jennifer Kidwell Drake
{"title":"塞内加尔自注射DMPA-SC与卫生工作者注射DMPA-IM的成本效益比较","authors":"Mercy Mvundura , Laura Di Giorgio , Chloe Morozoff , Jane Cover , Marguerite Ndour , Jennifer Kidwell Drake","doi":"10.1016/j.conx.2019.100012","DOIUrl":null,"url":null,"abstract":"<div><h3>Objectives</h3><p>To evaluate the cost-effectiveness of self-injected subcutaneous depot medroxyprogesterone acetate (DMPA-SC) compared to health-worker-administered intramuscular DMPA (DMPA-IM) in Senegal and to assess how including practice or demonstration injections in client self-injection training affects estimates.</p></div><div><h3>Study design</h3><p>We developed a decision-tree model with a 12-month time horizon for a hypothetical cohort of 100,000 injectable contraceptive users in Senegal. We used the model to estimate incremental costs per disability-adjusted life year (DALY) averted. The analysis derived model inputs from DMPA-SC self-injection continuation and costing research studies and peer-reviewed literature. We evaluated the cost-effectiveness from societal and health system perspectives and conducted one-way and probabilistic sensitivity analyses to test the robustness of results.</p></div><div><h3>Results</h3><p>Compared to health-worker-administered DMPA-IM, self-injected DMPA-SC could prevent 1402 additional unintended pregnancies and avert 204 maternal DALYs per year for this hypothetical cohort. From a societal perspective, self-injection costs less than health worker administration regardless of the training approach and is therefore dominant. From the health system perspective, self-injection is dominant compared to health worker administration if a one-page instruction sheet is used and one additional DMPA-SC unit is used for training and is cost-effective at $208 per DALY averted when two additional DMPA-SC units are used. Sensitivity analysis showed estimates were robust.</p></div><div><h3>Conclusions</h3><p>Self-injected DMPA-SC averted more pregnancies and DALYs and cost less from the societal perspective compared to health-worker-administered DMPA-IM and hence is dominant. Using fewer DMPA-SC units for practice or demonstration improves cost-effectiveness of self-injection from the health system perspective.</p></div><div><h3>Implications</h3><p>Evidence from Senegal shows that self-injection of DMPA-SC can be dominant or cost-effective from both health system and societal perspectives relative to DMPA-IM from health workers even if women practice injecting or health workers demonstrate with one or two DMPA-SC units. Evidence on whether practice or demonstration is required for client training would be useful.</p></div>","PeriodicalId":10655,"journal":{"name":"Contraception: X","volume":"1 ","pages":"Article 100012"},"PeriodicalIF":0.0000,"publicationDate":"2019-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1016/j.conx.2019.100012","citationCount":"4","resultStr":"{\"title\":\"Cost-effectiveness of self-injected DMPA-SC compared with health-worker-injected DMPA-IM in Senegal\",\"authors\":\"Mercy Mvundura , Laura Di Giorgio , Chloe Morozoff , Jane Cover , Marguerite Ndour , Jennifer Kidwell Drake\",\"doi\":\"10.1016/j.conx.2019.100012\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Objectives</h3><p>To evaluate the cost-effectiveness of self-injected subcutaneous depot medroxyprogesterone acetate (DMPA-SC) compared to health-worker-administered intramuscular DMPA (DMPA-IM) in Senegal and to assess how including practice or demonstration injections in client self-injection training affects estimates.</p></div><div><h3>Study design</h3><p>We developed a decision-tree model with a 12-month time horizon for a hypothetical cohort of 100,000 injectable contraceptive users in Senegal. We used the model to estimate incremental costs per disability-adjusted life year (DALY) averted. The analysis derived model inputs from DMPA-SC self-injection continuation and costing research studies and peer-reviewed literature. We evaluated the cost-effectiveness from societal and health system perspectives and conducted one-way and probabilistic sensitivity analyses to test the robustness of results.</p></div><div><h3>Results</h3><p>Compared to health-worker-administered DMPA-IM, self-injected DMPA-SC could prevent 1402 additional unintended pregnancies and avert 204 maternal DALYs per year for this hypothetical cohort. From a societal perspective, self-injection costs less than health worker administration regardless of the training approach and is therefore dominant. From the health system perspective, self-injection is dominant compared to health worker administration if a one-page instruction sheet is used and one additional DMPA-SC unit is used for training and is cost-effective at $208 per DALY averted when two additional DMPA-SC units are used. Sensitivity analysis showed estimates were robust.</p></div><div><h3>Conclusions</h3><p>Self-injected DMPA-SC averted more pregnancies and DALYs and cost less from the societal perspective compared to health-worker-administered DMPA-IM and hence is dominant. Using fewer DMPA-SC units for practice or demonstration improves cost-effectiveness of self-injection from the health system perspective.</p></div><div><h3>Implications</h3><p>Evidence from Senegal shows that self-injection of DMPA-SC can be dominant or cost-effective from both health system and societal perspectives relative to DMPA-IM from health workers even if women practice injecting or health workers demonstrate with one or two DMPA-SC units. Evidence on whether practice or demonstration is required for client training would be useful.</p></div>\",\"PeriodicalId\":10655,\"journal\":{\"name\":\"Contraception: X\",\"volume\":\"1 \",\"pages\":\"Article 100012\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2019-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1016/j.conx.2019.100012\",\"citationCount\":\"4\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Contraception: X\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2590151619300115\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Contraception: X","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2590151619300115","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
Cost-effectiveness of self-injected DMPA-SC compared with health-worker-injected DMPA-IM in Senegal
Objectives
To evaluate the cost-effectiveness of self-injected subcutaneous depot medroxyprogesterone acetate (DMPA-SC) compared to health-worker-administered intramuscular DMPA (DMPA-IM) in Senegal and to assess how including practice or demonstration injections in client self-injection training affects estimates.
Study design
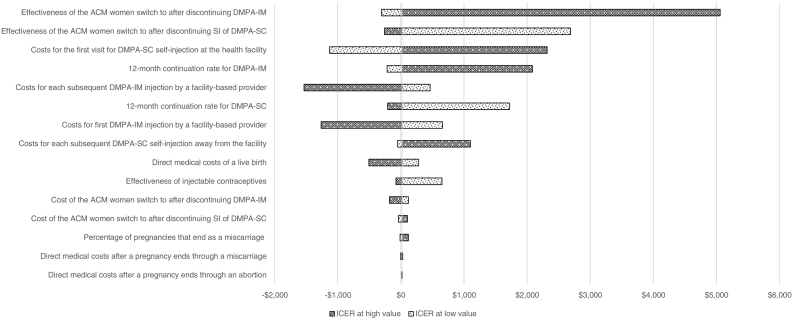
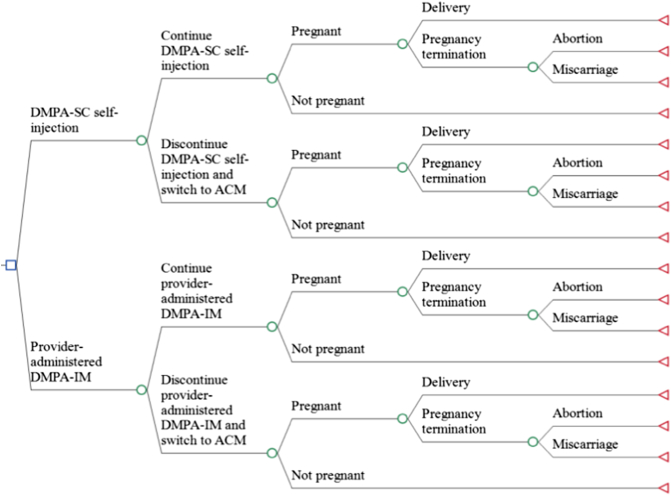
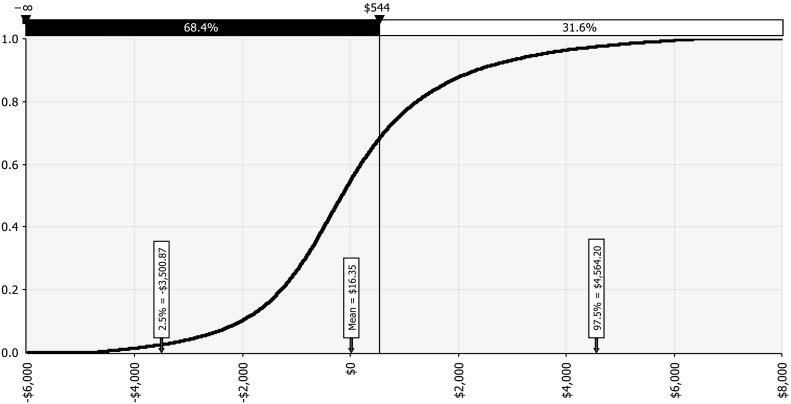
We developed a decision-tree model with a 12-month time horizon for a hypothetical cohort of 100,000 injectable contraceptive users in Senegal. We used the model to estimate incremental costs per disability-adjusted life year (DALY) averted. The analysis derived model inputs from DMPA-SC self-injection continuation and costing research studies and peer-reviewed literature. We evaluated the cost-effectiveness from societal and health system perspectives and conducted one-way and probabilistic sensitivity analyses to test the robustness of results.
Results
Compared to health-worker-administered DMPA-IM, self-injected DMPA-SC could prevent 1402 additional unintended pregnancies and avert 204 maternal DALYs per year for this hypothetical cohort. From a societal perspective, self-injection costs less than health worker administration regardless of the training approach and is therefore dominant. From the health system perspective, self-injection is dominant compared to health worker administration if a one-page instruction sheet is used and one additional DMPA-SC unit is used for training and is cost-effective at $208 per DALY averted when two additional DMPA-SC units are used. Sensitivity analysis showed estimates were robust.
Conclusions
Self-injected DMPA-SC averted more pregnancies and DALYs and cost less from the societal perspective compared to health-worker-administered DMPA-IM and hence is dominant. Using fewer DMPA-SC units for practice or demonstration improves cost-effectiveness of self-injection from the health system perspective.
Implications
Evidence from Senegal shows that self-injection of DMPA-SC can be dominant or cost-effective from both health system and societal perspectives relative to DMPA-IM from health workers even if women practice injecting or health workers demonstrate with one or two DMPA-SC units. Evidence on whether practice or demonstration is required for client training would be useful.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


