Suhas Rao, Anoop T Chakrapani, Ashok Kumar Uppiretla, Donnel Don Bosco
{"title":"没有结构性心脏病的年轻女孩的电风暴。","authors":"Suhas Rao, Anoop T Chakrapani, Ashok Kumar Uppiretla, Donnel Don Bosco","doi":"10.22114/ajem.v0i0.221","DOIUrl":null,"url":null,"abstract":"A 14-year-old girl presented to the emergency department (ED) with a history of three episodes of seizure-like activity and no comorbidities at 2 am. The first episode had occurred at 6 am, the second at 12 pm and the third two hours before presenting to the ED. Each episode lasting less than 5 minutes, was associated with the limb and spinal rigidity and extension, the up-rolling of eyeballs and urinary incontinence. The patient reported no history of fever, recent trauma, previous febrile seizures, prodromal symptoms, tongue bite, headache or physical excretion before the episodes. No postictal confusion or tonic-clonic movements and significant family history were also reported. The initial examination found her to be conscious, oriented and hemodynamically stable, and the results of her systemic examinations were normal without any significant positive findings. \nEvaluation of the patient initiated with the provisional diagnosis of new-onset seizures, followed by performing a computed tomography (CT) scan of the head, which was normal and ruled out any intra-cranial pathology. The results of the blood test involving serum electrolytes, calcium and magnesium were also normal. \nAbrupt polymorphic ventricular tachycardia (VT) was identified on the monitor (figure 1) as a few second-episodes of posturing and stretching of the body with no peripheral and central pulses during the examination in the ED. The patient came around after undergoing cardiopulmonary resuscitation immediately followed by defibrillation at 200 J and reverting the rhythm to sinus. The patient had recurrent episodes of pulseless polymorphic VT, which required ten times of defibrillation for one hour and antiarrhythmic drug therapy with IV bolus of 300 mg and then again 150 mg amidaraone, and then infusion of 1 mg of magnesium sulfate diluted in 10 ml of D5W and also administration of 1 mg/kg of lidocaine. \nThe patient was electively intubated and ventilated under deep sedation, and transferred to the cardiac care unit (CCU). The two-dimensional echocardiography findings were revealed normal-sized heart chambers and good left ventricular function. Blood levels of high-sensitivity troponin I and CK-MB were also in their normal range. Despite performing repeated defibrillation and anti-arrhythmic therapy, the patient showed repeated episodes of pulseless VT. She was therefore referred to a higher-level center to be administered with left stellate ganglion block (LSGB). She withstood the procedure, and discharged from the hospital after a ten-day follow-up. An implantable cardioverter-defibrillator (ICD) was later planned for the patient, and she continued with taking oral antiarrhythmic drugs.","PeriodicalId":7290,"journal":{"name":"Advanced Journal of Emergency Medicine","volume":"4 1","pages":"e14"},"PeriodicalIF":0.0000,"publicationDate":"2019-09-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/4b/70/AJEM-4-e14.PMC6955023.pdf","citationCount":"0","resultStr":"{\"title\":\"Electrical Storm in the Absence of a Structural Heart Disease in a Young Girl.\",\"authors\":\"Suhas Rao, Anoop T Chakrapani, Ashok Kumar Uppiretla, Donnel Don Bosco\",\"doi\":\"10.22114/ajem.v0i0.221\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"A 14-year-old girl presented to the emergency department (ED) with a history of three episodes of seizure-like activity and no comorbidities at 2 am. The first episode had occurred at 6 am, the second at 12 pm and the third two hours before presenting to the ED. Each episode lasting less than 5 minutes, was associated with the limb and spinal rigidity and extension, the up-rolling of eyeballs and urinary incontinence. The patient reported no history of fever, recent trauma, previous febrile seizures, prodromal symptoms, tongue bite, headache or physical excretion before the episodes. No postictal confusion or tonic-clonic movements and significant family history were also reported. The initial examination found her to be conscious, oriented and hemodynamically stable, and the results of her systemic examinations were normal without any significant positive findings. \\nEvaluation of the patient initiated with the provisional diagnosis of new-onset seizures, followed by performing a computed tomography (CT) scan of the head, which was normal and ruled out any intra-cranial pathology. The results of the blood test involving serum electrolytes, calcium and magnesium were also normal. \\nAbrupt polymorphic ventricular tachycardia (VT) was identified on the monitor (figure 1) as a few second-episodes of posturing and stretching of the body with no peripheral and central pulses during the examination in the ED. The patient came around after undergoing cardiopulmonary resuscitation immediately followed by defibrillation at 200 J and reverting the rhythm to sinus. The patient had recurrent episodes of pulseless polymorphic VT, which required ten times of defibrillation for one hour and antiarrhythmic drug therapy with IV bolus of 300 mg and then again 150 mg amidaraone, and then infusion of 1 mg of magnesium sulfate diluted in 10 ml of D5W and also administration of 1 mg/kg of lidocaine. \\nThe patient was electively intubated and ventilated under deep sedation, and transferred to the cardiac care unit (CCU). The two-dimensional echocardiography findings were revealed normal-sized heart chambers and good left ventricular function. Blood levels of high-sensitivity troponin I and CK-MB were also in their normal range. Despite performing repeated defibrillation and anti-arrhythmic therapy, the patient showed repeated episodes of pulseless VT. She was therefore referred to a higher-level center to be administered with left stellate ganglion block (LSGB). She withstood the procedure, and discharged from the hospital after a ten-day follow-up. An implantable cardioverter-defibrillator (ICD) was later planned for the patient, and she continued with taking oral antiarrhythmic drugs.\",\"PeriodicalId\":7290,\"journal\":{\"name\":\"Advanced Journal of Emergency Medicine\",\"volume\":\"4 1\",\"pages\":\"e14\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2019-09-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/4b/70/AJEM-4-e14.PMC6955023.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Advanced Journal of Emergency Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.22114/ajem.v0i0.221\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Advanced Journal of Emergency Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.22114/ajem.v0i0.221","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Electrical Storm in the Absence of a Structural Heart Disease in a Young Girl.
A 14-year-old girl presented to the emergency department (ED) with a history of three episodes of seizure-like activity and no comorbidities at 2 am. The first episode had occurred at 6 am, the second at 12 pm and the third two hours before presenting to the ED. Each episode lasting less than 5 minutes, was associated with the limb and spinal rigidity and extension, the up-rolling of eyeballs and urinary incontinence. The patient reported no history of fever, recent trauma, previous febrile seizures, prodromal symptoms, tongue bite, headache or physical excretion before the episodes. No postictal confusion or tonic-clonic movements and significant family history were also reported. The initial examination found her to be conscious, oriented and hemodynamically stable, and the results of her systemic examinations were normal without any significant positive findings.
Evaluation of the patient initiated with the provisional diagnosis of new-onset seizures, followed by performing a computed tomography (CT) scan of the head, which was normal and ruled out any intra-cranial pathology. The results of the blood test involving serum electrolytes, calcium and magnesium were also normal.
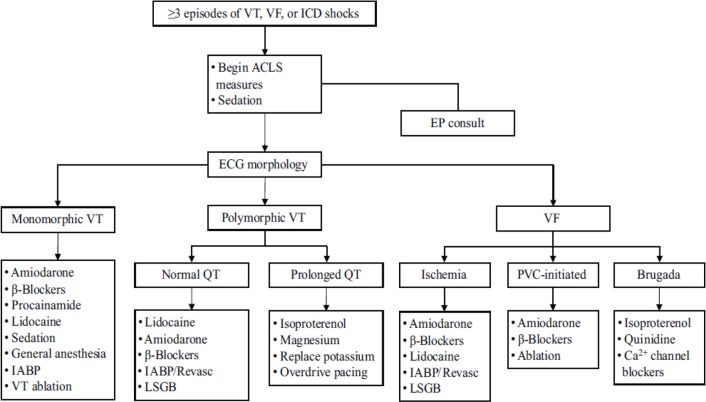
Abrupt polymorphic ventricular tachycardia (VT) was identified on the monitor (figure 1) as a few second-episodes of posturing and stretching of the body with no peripheral and central pulses during the examination in the ED. The patient came around after undergoing cardiopulmonary resuscitation immediately followed by defibrillation at 200 J and reverting the rhythm to sinus. The patient had recurrent episodes of pulseless polymorphic VT, which required ten times of defibrillation for one hour and antiarrhythmic drug therapy with IV bolus of 300 mg and then again 150 mg amidaraone, and then infusion of 1 mg of magnesium sulfate diluted in 10 ml of D5W and also administration of 1 mg/kg of lidocaine.
The patient was electively intubated and ventilated under deep sedation, and transferred to the cardiac care unit (CCU). The two-dimensional echocardiography findings were revealed normal-sized heart chambers and good left ventricular function. Blood levels of high-sensitivity troponin I and CK-MB were also in their normal range. Despite performing repeated defibrillation and anti-arrhythmic therapy, the patient showed repeated episodes of pulseless VT. She was therefore referred to a higher-level center to be administered with left stellate ganglion block (LSGB). She withstood the procedure, and discharged from the hospital after a ten-day follow-up. An implantable cardioverter-defibrillator (ICD) was later planned for the patient, and she continued with taking oral antiarrhythmic drugs.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


