{"title":"扩张型心肌病女性双向室性心动过速1例报告。","authors":"Dalton Argean Norwood, Lucia Belem Dominguez, Ricardo Leonel Dominguez, Walter Tyler Winders","doi":"10.22114/ajem.v0i0.287","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Bidirectional ventricular tachycardia (BVT) is a rare arrhythmia characterized by QRS complexes with an axis in the frontal plane alternating polarity in the precordial leads and right bundle branch block (RBBB) morphology. To the best of our knowledge, there is no previous report in dilated cardiomyopathy or in the context of a probable peripartum cardiomyopathy.</p><p><strong>Case presentation: </strong>A 26-year-old, 9-month female patient, with no significant past medical history (the patient denies medication intake, herbs like aconite, trouble during delivery, any heart issues or family history of sudden death or cardiomyopathies) who presents to the emergency room due to 11 days of dyspnea, exacerbated by daily activities, orthopnea, and paroxysmal nocturnal dyspnea. She presented with ventricular bigeminy and systolic dysfunction with left ventricular ejection fraction (LVEF) <20%. The patient later developed a stable ventricular tachycardia (VT) treated with amiodarone, which resulted in hemodynamic instability and BVT rhythm with VT paroxysms. Without the possibility of ablation, the use of high dose beta blockers and an implantable cardioverter defibrillator resulted in the same rhythm with a lower heart rate, better NYHA functional class, and less episodes of VTs.</p><p><strong>Conclusion: </strong>BVT is a rare type of tachycardia that can be present in dilated cardiomyopathy. In the absence of ablation capabilities, decreasing the heart rate with beta-blockers may reduce the rate of paroxysmal VTs.</p>","PeriodicalId":7290,"journal":{"name":"Advanced Journal of Emergency Medicine","volume":"4 1","pages":"e12"},"PeriodicalIF":0.0000,"publicationDate":"2019-10-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/73/7c/AJEM-4-e12.PMC6955033.pdf","citationCount":"1","resultStr":"{\"title\":\"Bidirectional Ventricular Tachycardia in a Women with Dilated Cardiomyopathy: A Case Report.\",\"authors\":\"Dalton Argean Norwood, Lucia Belem Dominguez, Ricardo Leonel Dominguez, Walter Tyler Winders\",\"doi\":\"10.22114/ajem.v0i0.287\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Bidirectional ventricular tachycardia (BVT) is a rare arrhythmia characterized by QRS complexes with an axis in the frontal plane alternating polarity in the precordial leads and right bundle branch block (RBBB) morphology. To the best of our knowledge, there is no previous report in dilated cardiomyopathy or in the context of a probable peripartum cardiomyopathy.</p><p><strong>Case presentation: </strong>A 26-year-old, 9-month female patient, with no significant past medical history (the patient denies medication intake, herbs like aconite, trouble during delivery, any heart issues or family history of sudden death or cardiomyopathies) who presents to the emergency room due to 11 days of dyspnea, exacerbated by daily activities, orthopnea, and paroxysmal nocturnal dyspnea. She presented with ventricular bigeminy and systolic dysfunction with left ventricular ejection fraction (LVEF) <20%. The patient later developed a stable ventricular tachycardia (VT) treated with amiodarone, which resulted in hemodynamic instability and BVT rhythm with VT paroxysms. Without the possibility of ablation, the use of high dose beta blockers and an implantable cardioverter defibrillator resulted in the same rhythm with a lower heart rate, better NYHA functional class, and less episodes of VTs.</p><p><strong>Conclusion: </strong>BVT is a rare type of tachycardia that can be present in dilated cardiomyopathy. In the absence of ablation capabilities, decreasing the heart rate with beta-blockers may reduce the rate of paroxysmal VTs.</p>\",\"PeriodicalId\":7290,\"journal\":{\"name\":\"Advanced Journal of Emergency Medicine\",\"volume\":\"4 1\",\"pages\":\"e12\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2019-10-31\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/73/7c/AJEM-4-e12.PMC6955033.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Advanced Journal of Emergency Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.22114/ajem.v0i0.287\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Advanced Journal of Emergency Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.22114/ajem.v0i0.287","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Bidirectional Ventricular Tachycardia in a Women with Dilated Cardiomyopathy: A Case Report.
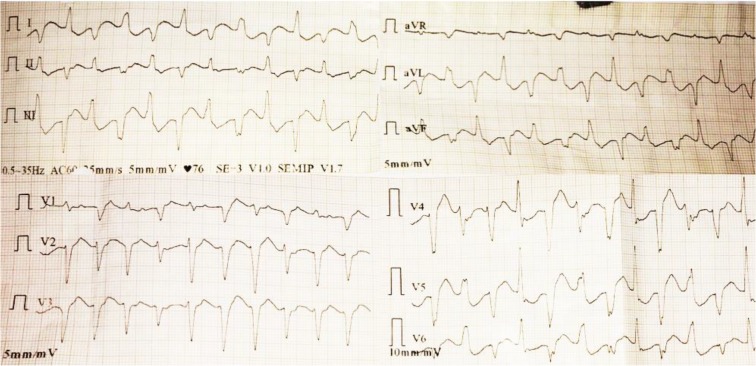
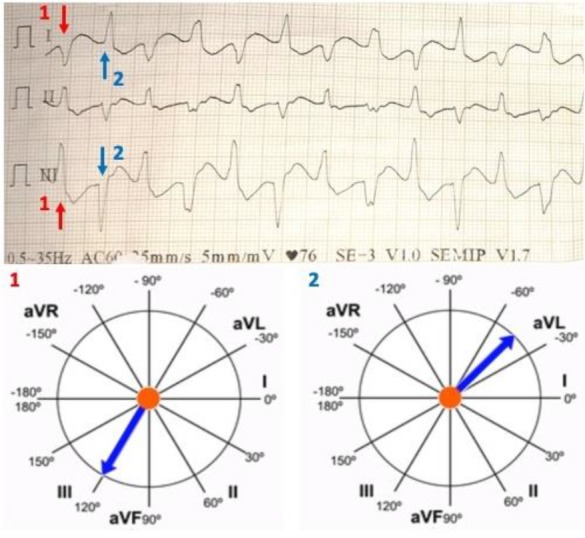
Introduction: Bidirectional ventricular tachycardia (BVT) is a rare arrhythmia characterized by QRS complexes with an axis in the frontal plane alternating polarity in the precordial leads and right bundle branch block (RBBB) morphology. To the best of our knowledge, there is no previous report in dilated cardiomyopathy or in the context of a probable peripartum cardiomyopathy.
Case presentation: A 26-year-old, 9-month female patient, with no significant past medical history (the patient denies medication intake, herbs like aconite, trouble during delivery, any heart issues or family history of sudden death or cardiomyopathies) who presents to the emergency room due to 11 days of dyspnea, exacerbated by daily activities, orthopnea, and paroxysmal nocturnal dyspnea. She presented with ventricular bigeminy and systolic dysfunction with left ventricular ejection fraction (LVEF) <20%. The patient later developed a stable ventricular tachycardia (VT) treated with amiodarone, which resulted in hemodynamic instability and BVT rhythm with VT paroxysms. Without the possibility of ablation, the use of high dose beta blockers and an implantable cardioverter defibrillator resulted in the same rhythm with a lower heart rate, better NYHA functional class, and less episodes of VTs.
Conclusion: BVT is a rare type of tachycardia that can be present in dilated cardiomyopathy. In the absence of ablation capabilities, decreasing the heart rate with beta-blockers may reduce the rate of paroxysmal VTs.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


