Clara K Chow, David Brieger, Mark Ryan, Nadarajah Kangaharan, Karice K Hyun, Tom Briffa
{"title":"急性冠脉综合征的二级预防治疗及其与预后的关系:观察性研究。","authors":"Clara K Chow, David Brieger, Mark Ryan, Nadarajah Kangaharan, Karice K Hyun, Tom Briffa","doi":"10.1136/heartasia-2018-011122","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To ascertain the use of secondary prevention medications and cardiac rehabilitation after an acute coronary syndrome (ACS) and the impact on 2-year outcomes.</p><p><strong>Methods: </strong>CONCORDANCE (Cooperative National Registry of Acute Coronary care, Guideline Adherence and Clinical Events) is a prospective, observational registry of 41 Australian hospitals. A representative sample of 6859 patients with an ACS and 6 months' follow-up on 31 May 2016 were included. The main outcome measure was use of ≥75% of indicated medications (≥4/5 (or ≥3/4 if contraindicated) of angiotensin-converting enzyme (ACE) inhibitor/angiotensin receptor blocker, beta-blocker, lipid-lowering therapy, aspirin and other antiplatelet). Major adverse cardiovascular events (MACE) included myocardial infarction, stroke or cardiovascular death.</p><p><strong>Results: </strong>The mean age was 65±13 years, 29% were women, and the mean Global Registry of Acute Coronary Events (GRACE) score was 106±30. At discharge, 92% were on aspirin, 93% lipid-lowering therapy, 78% beta-blocker, 74% ACE/angiotensin receptor blocker and 73% a second antiplatelet; 89% were taking ≥75% of medications at discharge, 78% at 6 months and 66% at 2 years. At 6 months, 38% attended cardiac rehabilitation, 58% received dietary advice and 32% of smokers reported quitting. Among 1896 patients followed to 2 years, death/MACE was less frequent among patients on ≥75% vs <75% of medications (8.3% vs 13.9%; adjusted OR 0.75, 95 % CI 0.56 to 0.99), and was less frequent in patients who attended versus who did not attend cardiac rehabilitation (4.6% vs 13.4%; adjusted OR 0.44, 95% CI 0.31 to 0.62).</p><p><strong>Conclusions: </strong>Use of secondary prevention therapies diminishes over time following an ACS. Patients receiving secondary prevention had decreased rates of death and MACE at 2 years.</p>","PeriodicalId":12858,"journal":{"name":"Heart Asia","volume":"11 1","pages":"e011122"},"PeriodicalIF":0.0000,"publicationDate":"2019-01-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1136/heartasia-2018-011122","citationCount":"16","resultStr":"{\"title\":\"Secondary prevention therapies in acute coronary syndrome and relation to outcomes: observational study.\",\"authors\":\"Clara K Chow, David Brieger, Mark Ryan, Nadarajah Kangaharan, Karice K Hyun, Tom Briffa\",\"doi\":\"10.1136/heartasia-2018-011122\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>To ascertain the use of secondary prevention medications and cardiac rehabilitation after an acute coronary syndrome (ACS) and the impact on 2-year outcomes.</p><p><strong>Methods: </strong>CONCORDANCE (Cooperative National Registry of Acute Coronary care, Guideline Adherence and Clinical Events) is a prospective, observational registry of 41 Australian hospitals. A representative sample of 6859 patients with an ACS and 6 months' follow-up on 31 May 2016 were included. The main outcome measure was use of ≥75% of indicated medications (≥4/5 (or ≥3/4 if contraindicated) of angiotensin-converting enzyme (ACE) inhibitor/angiotensin receptor blocker, beta-blocker, lipid-lowering therapy, aspirin and other antiplatelet). Major adverse cardiovascular events (MACE) included myocardial infarction, stroke or cardiovascular death.</p><p><strong>Results: </strong>The mean age was 65±13 years, 29% were women, and the mean Global Registry of Acute Coronary Events (GRACE) score was 106±30. At discharge, 92% were on aspirin, 93% lipid-lowering therapy, 78% beta-blocker, 74% ACE/angiotensin receptor blocker and 73% a second antiplatelet; 89% were taking ≥75% of medications at discharge, 78% at 6 months and 66% at 2 years. At 6 months, 38% attended cardiac rehabilitation, 58% received dietary advice and 32% of smokers reported quitting. Among 1896 patients followed to 2 years, death/MACE was less frequent among patients on ≥75% vs <75% of medications (8.3% vs 13.9%; adjusted OR 0.75, 95 % CI 0.56 to 0.99), and was less frequent in patients who attended versus who did not attend cardiac rehabilitation (4.6% vs 13.4%; adjusted OR 0.44, 95% CI 0.31 to 0.62).</p><p><strong>Conclusions: </strong>Use of secondary prevention therapies diminishes over time following an ACS. Patients receiving secondary prevention had decreased rates of death and MACE at 2 years.</p>\",\"PeriodicalId\":12858,\"journal\":{\"name\":\"Heart Asia\",\"volume\":\"11 1\",\"pages\":\"e011122\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2019-01-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1136/heartasia-2018-011122\",\"citationCount\":\"16\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Heart Asia\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1136/heartasia-2018-011122\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2019/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Heart Asia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/heartasia-2018-011122","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2019/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
Secondary prevention therapies in acute coronary syndrome and relation to outcomes: observational study.
Objective: To ascertain the use of secondary prevention medications and cardiac rehabilitation after an acute coronary syndrome (ACS) and the impact on 2-year outcomes.
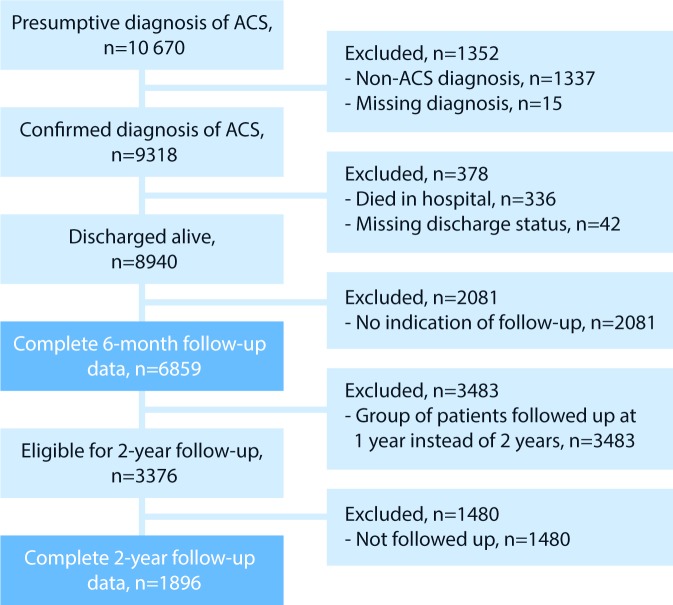
Methods: CONCORDANCE (Cooperative National Registry of Acute Coronary care, Guideline Adherence and Clinical Events) is a prospective, observational registry of 41 Australian hospitals. A representative sample of 6859 patients with an ACS and 6 months' follow-up on 31 May 2016 were included. The main outcome measure was use of ≥75% of indicated medications (≥4/5 (or ≥3/4 if contraindicated) of angiotensin-converting enzyme (ACE) inhibitor/angiotensin receptor blocker, beta-blocker, lipid-lowering therapy, aspirin and other antiplatelet). Major adverse cardiovascular events (MACE) included myocardial infarction, stroke or cardiovascular death.
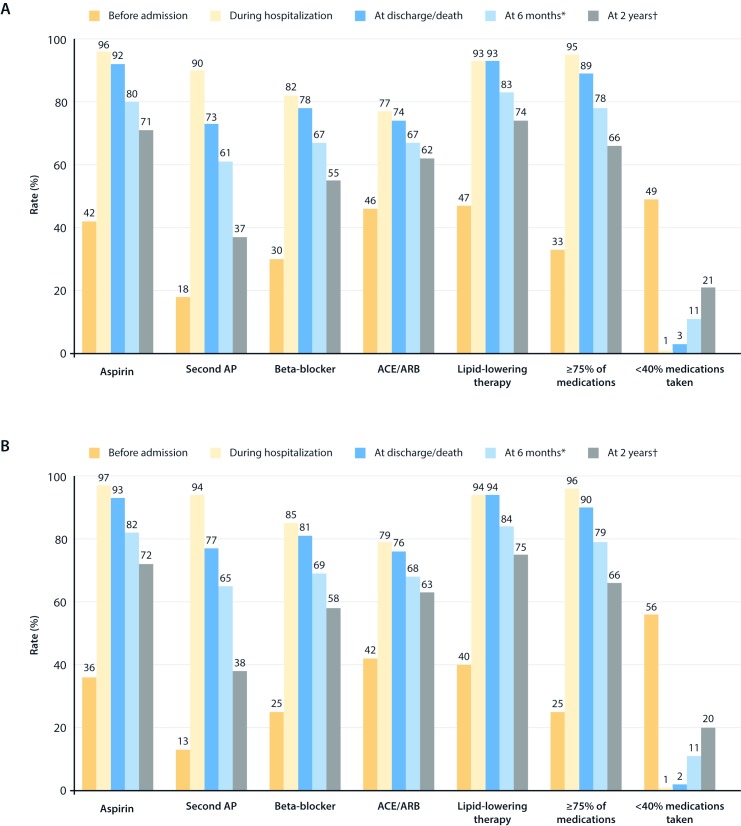
Results: The mean age was 65±13 years, 29% were women, and the mean Global Registry of Acute Coronary Events (GRACE) score was 106±30. At discharge, 92% were on aspirin, 93% lipid-lowering therapy, 78% beta-blocker, 74% ACE/angiotensin receptor blocker and 73% a second antiplatelet; 89% were taking ≥75% of medications at discharge, 78% at 6 months and 66% at 2 years. At 6 months, 38% attended cardiac rehabilitation, 58% received dietary advice and 32% of smokers reported quitting. Among 1896 patients followed to 2 years, death/MACE was less frequent among patients on ≥75% vs <75% of medications (8.3% vs 13.9%; adjusted OR 0.75, 95 % CI 0.56 to 0.99), and was less frequent in patients who attended versus who did not attend cardiac rehabilitation (4.6% vs 13.4%; adjusted OR 0.44, 95% CI 0.31 to 0.62).
Conclusions: Use of secondary prevention therapies diminishes over time following an ACS. Patients receiving secondary prevention had decreased rates of death and MACE at 2 years.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


