Saartje Straetemans, Muriel Thomas, Margarita Craen, Raoul Rooman, Jean De Schepper
{"title":"生长激素缺乏症和出生胎龄小的短青春期前儿童在生长激素治疗的第一年生长反应差:不同标准的比较","authors":"Saartje Straetemans, Muriel Thomas, Margarita Craen, Raoul Rooman, Jean De Schepper","doi":"10.1186/s13633-018-0064-3","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>There is no consensus on the definition of poor growth response after the first year of growth hormone (GH) treatment. We determined the proportion of poor responders identified by different criteria in children with GH deficiency (GHD) and born small for gestational age (SGA). The second aim was to analyze the IGF-1 response in poor growth responders.</p><p><strong>Methods: </strong>First-year height data of 171 SGA and 122 GHD children who remained prepubertal during the first GH treatment year were retrieved from the BESPEED database and analyzed. Criteria for poor first-year response/responsiveness were: change in height (∆Ht) SDS<0.3 or<0.5, height velocity (HV) SDS<0.5 or <1 based on the population reference, HV SDS<- 1 based on the KIGS expected HV curve (HV Ranke SDS), studentized residual (SR) <- 1 in the KIGS first-year prediction model.</p><p><strong>Results: </strong>∆Ht SDS<0.5 gave the highest percentage poor responders (37% SGA, 26% GHD). Although % poor responders were comparable for ∆Ht SDS<0.3, HV SDS<+ 0.5, HV SDS<+ 1, SR<- 1, and HV Ranke SDS<- 1, these criteria did not always identify the same patients as poor responders. Among the poor growth responders 24% SGA and 14% GHD patients had an IGF-1 increase < 40%.</p><p><strong>Conclusions: </strong>The different response criteria yield high but comparable percentages poor responders, but identify different patients. This study does not provide evidence that one criterion is better than another. A limited IGF-1 generation is not the major reason for a poor growth response in the first year of GH treatment in SGA and GHD children.</p><p><strong>Trial registration: </strong>Retrospectively registered.</p>","PeriodicalId":14271,"journal":{"name":"International Journal of Pediatric Endocrinology","volume":"2018 ","pages":"9"},"PeriodicalIF":0.0000,"publicationDate":"2018-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/s13633-018-0064-3","citationCount":"17","resultStr":"{\"title\":\"Poor growth response during the first year of growth hormone treatment in short prepubertal children with growth hormone deficiency and born small for gestational age: a comparison of different criteria.\",\"authors\":\"Saartje Straetemans, Muriel Thomas, Margarita Craen, Raoul Rooman, Jean De Schepper\",\"doi\":\"10.1186/s13633-018-0064-3\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>There is no consensus on the definition of poor growth response after the first year of growth hormone (GH) treatment. We determined the proportion of poor responders identified by different criteria in children with GH deficiency (GHD) and born small for gestational age (SGA). The second aim was to analyze the IGF-1 response in poor growth responders.</p><p><strong>Methods: </strong>First-year height data of 171 SGA and 122 GHD children who remained prepubertal during the first GH treatment year were retrieved from the BESPEED database and analyzed. Criteria for poor first-year response/responsiveness were: change in height (∆Ht) SDS<0.3 or<0.5, height velocity (HV) SDS<0.5 or <1 based on the population reference, HV SDS<- 1 based on the KIGS expected HV curve (HV Ranke SDS), studentized residual (SR) <- 1 in the KIGS first-year prediction model.</p><p><strong>Results: </strong>∆Ht SDS<0.5 gave the highest percentage poor responders (37% SGA, 26% GHD). Although % poor responders were comparable for ∆Ht SDS<0.3, HV SDS<+ 0.5, HV SDS<+ 1, SR<- 1, and HV Ranke SDS<- 1, these criteria did not always identify the same patients as poor responders. Among the poor growth responders 24% SGA and 14% GHD patients had an IGF-1 increase < 40%.</p><p><strong>Conclusions: </strong>The different response criteria yield high but comparable percentages poor responders, but identify different patients. This study does not provide evidence that one criterion is better than another. A limited IGF-1 generation is not the major reason for a poor growth response in the first year of GH treatment in SGA and GHD children.</p><p><strong>Trial registration: </strong>Retrospectively registered.</p>\",\"PeriodicalId\":14271,\"journal\":{\"name\":\"International Journal of Pediatric Endocrinology\",\"volume\":\"2018 \",\"pages\":\"9\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2018-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1186/s13633-018-0064-3\",\"citationCount\":\"17\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Journal of Pediatric Endocrinology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s13633-018-0064-3\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2018/10/22 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Pediatric Endocrinology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13633-018-0064-3","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2018/10/22 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Poor growth response during the first year of growth hormone treatment in short prepubertal children with growth hormone deficiency and born small for gestational age: a comparison of different criteria.
Background: There is no consensus on the definition of poor growth response after the first year of growth hormone (GH) treatment. We determined the proportion of poor responders identified by different criteria in children with GH deficiency (GHD) and born small for gestational age (SGA). The second aim was to analyze the IGF-1 response in poor growth responders.
Methods: First-year height data of 171 SGA and 122 GHD children who remained prepubertal during the first GH treatment year were retrieved from the BESPEED database and analyzed. Criteria for poor first-year response/responsiveness were: change in height (∆Ht) SDS<0.3 or<0.5, height velocity (HV) SDS<0.5 or <1 based on the population reference, HV SDS<- 1 based on the KIGS expected HV curve (HV Ranke SDS), studentized residual (SR) <- 1 in the KIGS first-year prediction model.
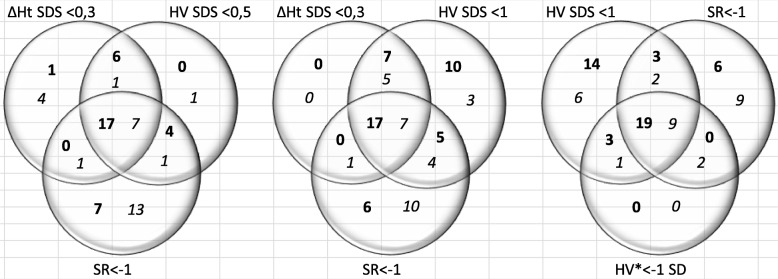
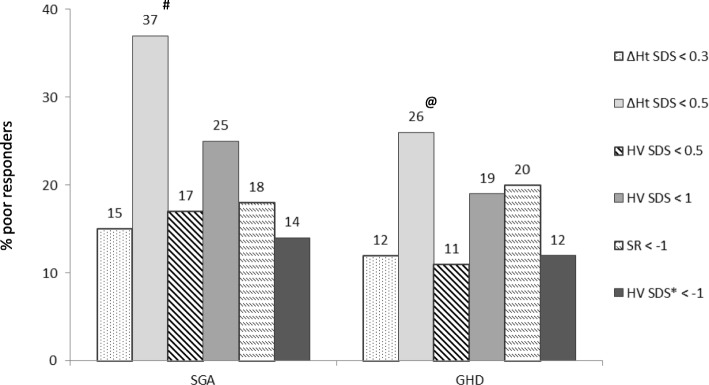
Results: ∆Ht SDS<0.5 gave the highest percentage poor responders (37% SGA, 26% GHD). Although % poor responders were comparable for ∆Ht SDS<0.3, HV SDS<+ 0.5, HV SDS<+ 1, SR<- 1, and HV Ranke SDS<- 1, these criteria did not always identify the same patients as poor responders. Among the poor growth responders 24% SGA and 14% GHD patients had an IGF-1 increase < 40%.
Conclusions: The different response criteria yield high but comparable percentages poor responders, but identify different patients. This study does not provide evidence that one criterion is better than another. A limited IGF-1 generation is not the major reason for a poor growth response in the first year of GH treatment in SGA and GHD children.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


