Ogugua Ndili Obi, Mark Mazer, Charles Bangley, Zuheir Kassabo, Khalid Saadah, Wayne Trainor, Kenneth Stephens, Patricia L Rice, Robert Shaw
{"title":"肥胖与机械通气脱机的探索性研究。","authors":"Ogugua Ndili Obi, Mark Mazer, Charles Bangley, Zuheir Kassabo, Khalid Saadah, Wayne Trainor, Kenneth Stephens, Patricia L Rice, Robert Shaw","doi":"10.1177/1179548418801004","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Obesity is associated with increased risk of hypercapnic respiratory failure, prolonged duration on mechanical ventilation, and extended weaning periods.</p><p><strong>Objective: </strong>Pilot study to determine whether morbidly obese adult tracheotomized subjects (body mass index [BMI] ⩾ 40) can be more efficiently weaned from the ventilator by optimizing their positive end-expiratory pressure (PEEP) using either an esophageal balloon or the best achieved static effective compliance.</p><p><strong>Methods: </strong>We randomly assigned 25 morbidly obese adult tracheotomized subjects (median [interquartile range] BMI 53.4 [26.4]; range 40.4-113.8) to 1 of 2 methods of setting PEEP; using either titration guided by esophageal balloon to overcome negative transpulmonary pressure (Ptp) (goal Ptp 0-5 cmH<sub>2</sub>O) (ESO group) or titration to maximize static effective lung compliance (Cstat group). Our outcomes of interest were number of subjects weaned by day 30 and time to wean.</p><p><strong>Results: </strong>At day 30, there was no significant difference in percentage of subjects weaned. 8/13 subjects (62%) in the ESO Group were weaned vs. 9/12(75%) in the Cstat Group (<i>P</i> = 0.67). Among the 17 subjects who weaned, median time to ventilator liberation was significantly shorter in the ESO group: 3.5 days vs Cstat group 14 days (<i>P</i> = .01). Optimal PEEP in the ESO and Cstat groups was similar (ESO mean ± SD = 26.5 ± 5.7 cmH<sub>2</sub>O and Cstat 24.2 ± 7 cmH<sub>2</sub>O (<i>P</i> = .38).</p><p><strong>Conclusions: </strong>Optimization of PEEP using esophageal balloon to achieve positive transpulmonary pressure did not change the proportion of patients weaned. Among patients who weaned, use of the esophageal balloon resulted in faster liberation from mechanical ventilation. There were no adverse consequences of the high PEEP (mean 25.4; range 13-37 cmH<sub>2</sub>O) used in our study. The study was approved by the Institutional Review Board at our institution (UMCIRB#10-0343) and registered with clinicaltrials.gov (NCT02323009).</p>","PeriodicalId":44269,"journal":{"name":"Clinical Medicine Insights-Circulatory Respiratory and Pulmonary Medicine","volume":"12 ","pages":"1179548418801004"},"PeriodicalIF":1.0000,"publicationDate":"2018-09-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1177/1179548418801004","citationCount":"10","resultStr":"{\"title\":\"Obesity and Weaning from Mechanical Ventilation-An Exploratory Study.\",\"authors\":\"Ogugua Ndili Obi, Mark Mazer, Charles Bangley, Zuheir Kassabo, Khalid Saadah, Wayne Trainor, Kenneth Stephens, Patricia L Rice, Robert Shaw\",\"doi\":\"10.1177/1179548418801004\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Obesity is associated with increased risk of hypercapnic respiratory failure, prolonged duration on mechanical ventilation, and extended weaning periods.</p><p><strong>Objective: </strong>Pilot study to determine whether morbidly obese adult tracheotomized subjects (body mass index [BMI] ⩾ 40) can be more efficiently weaned from the ventilator by optimizing their positive end-expiratory pressure (PEEP) using either an esophageal balloon or the best achieved static effective compliance.</p><p><strong>Methods: </strong>We randomly assigned 25 morbidly obese adult tracheotomized subjects (median [interquartile range] BMI 53.4 [26.4]; range 40.4-113.8) to 1 of 2 methods of setting PEEP; using either titration guided by esophageal balloon to overcome negative transpulmonary pressure (Ptp) (goal Ptp 0-5 cmH<sub>2</sub>O) (ESO group) or titration to maximize static effective lung compliance (Cstat group). Our outcomes of interest were number of subjects weaned by day 30 and time to wean.</p><p><strong>Results: </strong>At day 30, there was no significant difference in percentage of subjects weaned. 8/13 subjects (62%) in the ESO Group were weaned vs. 9/12(75%) in the Cstat Group (<i>P</i> = 0.67). Among the 17 subjects who weaned, median time to ventilator liberation was significantly shorter in the ESO group: 3.5 days vs Cstat group 14 days (<i>P</i> = .01). Optimal PEEP in the ESO and Cstat groups was similar (ESO mean ± SD = 26.5 ± 5.7 cmH<sub>2</sub>O and Cstat 24.2 ± 7 cmH<sub>2</sub>O (<i>P</i> = .38).</p><p><strong>Conclusions: </strong>Optimization of PEEP using esophageal balloon to achieve positive transpulmonary pressure did not change the proportion of patients weaned. Among patients who weaned, use of the esophageal balloon resulted in faster liberation from mechanical ventilation. There were no adverse consequences of the high PEEP (mean 25.4; range 13-37 cmH<sub>2</sub>O) used in our study. The study was approved by the Institutional Review Board at our institution (UMCIRB#10-0343) and registered with clinicaltrials.gov (NCT02323009).</p>\",\"PeriodicalId\":44269,\"journal\":{\"name\":\"Clinical Medicine Insights-Circulatory Respiratory and Pulmonary Medicine\",\"volume\":\"12 \",\"pages\":\"1179548418801004\"},\"PeriodicalIF\":1.0000,\"publicationDate\":\"2018-09-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1177/1179548418801004\",\"citationCount\":\"10\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Medicine Insights-Circulatory Respiratory and Pulmonary Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/1179548418801004\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2018/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine Insights-Circulatory Respiratory and Pulmonary Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/1179548418801004","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2018/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
Obesity and Weaning from Mechanical Ventilation-An Exploratory Study.
Introduction: Obesity is associated with increased risk of hypercapnic respiratory failure, prolonged duration on mechanical ventilation, and extended weaning periods.
Objective: Pilot study to determine whether morbidly obese adult tracheotomized subjects (body mass index [BMI] ⩾ 40) can be more efficiently weaned from the ventilator by optimizing their positive end-expiratory pressure (PEEP) using either an esophageal balloon or the best achieved static effective compliance.
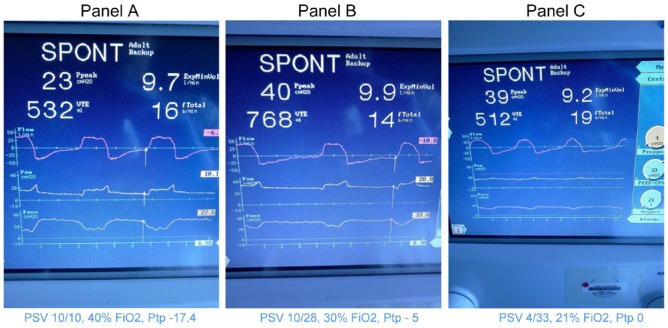
Methods: We randomly assigned 25 morbidly obese adult tracheotomized subjects (median [interquartile range] BMI 53.4 [26.4]; range 40.4-113.8) to 1 of 2 methods of setting PEEP; using either titration guided by esophageal balloon to overcome negative transpulmonary pressure (Ptp) (goal Ptp 0-5 cmH2O) (ESO group) or titration to maximize static effective lung compliance (Cstat group). Our outcomes of interest were number of subjects weaned by day 30 and time to wean.
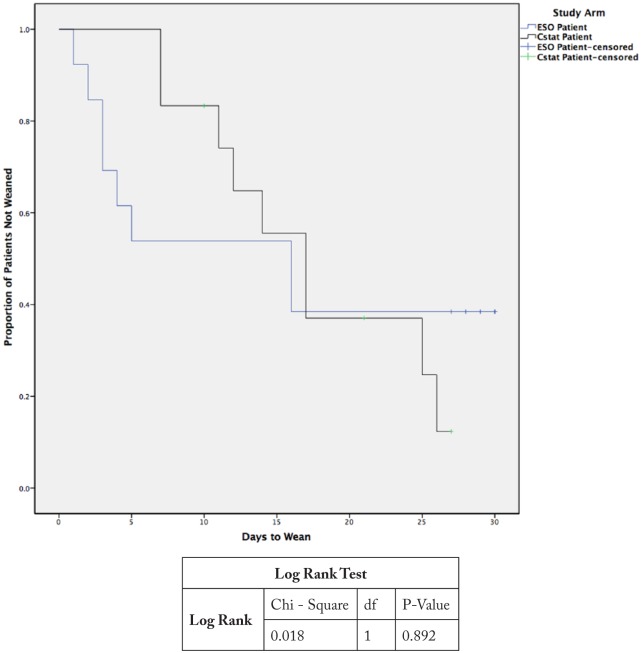
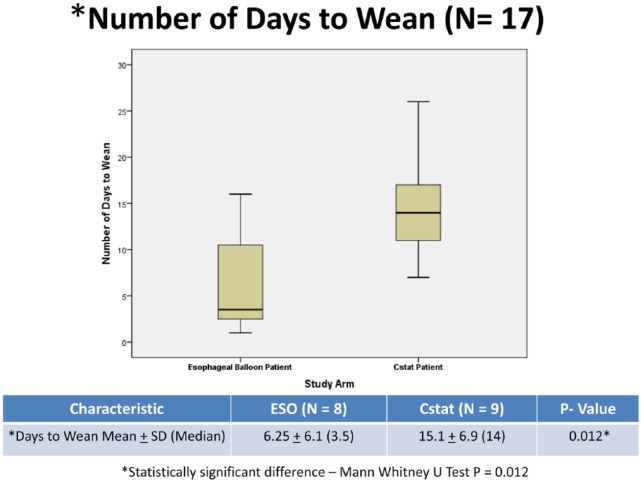
Results: At day 30, there was no significant difference in percentage of subjects weaned. 8/13 subjects (62%) in the ESO Group were weaned vs. 9/12(75%) in the Cstat Group (P = 0.67). Among the 17 subjects who weaned, median time to ventilator liberation was significantly shorter in the ESO group: 3.5 days vs Cstat group 14 days (P = .01). Optimal PEEP in the ESO and Cstat groups was similar (ESO mean ± SD = 26.5 ± 5.7 cmH2O and Cstat 24.2 ± 7 cmH2O (P = .38).
Conclusions: Optimization of PEEP using esophageal balloon to achieve positive transpulmonary pressure did not change the proportion of patients weaned. Among patients who weaned, use of the esophageal balloon resulted in faster liberation from mechanical ventilation. There were no adverse consequences of the high PEEP (mean 25.4; range 13-37 cmH2O) used in our study. The study was approved by the Institutional Review Board at our institution (UMCIRB#10-0343) and registered with clinicaltrials.gov (NCT02323009).

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


