Entidhar Al Sawah, Jason L Salemi, Mitchel Hoffman, Anthony N Imudia, Emad Mikhail
{"title":"子宫癌患者肥胖、手术方式和围手术期预后的关系","authors":"Entidhar Al Sawah, Jason L Salemi, Mitchel Hoffman, Anthony N Imudia, Emad Mikhail","doi":"10.1155/2018/5130856","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To study temporal trends of hysterectomy routes performed for uterine cancer and their associations with body mass index (BMI) and perioperative morbidity.</p><p><strong>Methods: </strong>A retrospective review of the American College of Surgeons-National Surgical Quality Improvement Program (ACS-NSQIP) 2005-2013 databases was conducted. All patients who were 18 years old and older with a diagnosis of uterine cancer and underwent hysterectomy were identified using ICD-9-CM and CPT codes. Surgical route was classified into four groups: total abdominal hysterectomy (TAH), total vaginal hysterectomy (TVH), laparoscopic assisted vaginal hysterectomy (LAVH), and total laparoscopic hysterectomy (TLH) including both conventional and robotically assisted. Patients were then stratified according to BMI.</p><p><strong>Results: </strong>7199 records were included in the study. TLH was the most commonly performed route of hysterectomy regardless of BMI, with proportions of 50.9%, 48.9%, 50.4%, and 51.2% in ideal, overweight, obese, and morbidly obese patients, respectively. The median operative time for TAH was 2.2 hours compared to 2.7 hours for TLH (<i>p</i> < 0.01). The median length of stay for TAH was 3 days compared to 1 day for TLH (<i>p</i> < 0.01). The percentage of patients with an adverse outcome (composite indicator including transfusion, deep venous thrombosis, and infection) was 17.1 versus 3.7 for TAH and TLH, respectively (<i>p</i> < 0.01).</p><p><strong>Conclusion: </strong>During the last decade, TLH has been increasingly performed in women with uterine cancer. The increased adoption of TLH was seen in all BMI subgroups.</p>","PeriodicalId":45110,"journal":{"name":"Minimally Invasive Surgery","volume":"2018 ","pages":"5130856"},"PeriodicalIF":1.3000,"publicationDate":"2018-06-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2018/5130856","citationCount":"12","resultStr":"{\"title\":\"Association between Obesity, Surgical Route, and Perioperative Outcomes in Patients with Uterine Cancer.\",\"authors\":\"Entidhar Al Sawah, Jason L Salemi, Mitchel Hoffman, Anthony N Imudia, Emad Mikhail\",\"doi\":\"10.1155/2018/5130856\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>To study temporal trends of hysterectomy routes performed for uterine cancer and their associations with body mass index (BMI) and perioperative morbidity.</p><p><strong>Methods: </strong>A retrospective review of the American College of Surgeons-National Surgical Quality Improvement Program (ACS-NSQIP) 2005-2013 databases was conducted. All patients who were 18 years old and older with a diagnosis of uterine cancer and underwent hysterectomy were identified using ICD-9-CM and CPT codes. Surgical route was classified into four groups: total abdominal hysterectomy (TAH), total vaginal hysterectomy (TVH), laparoscopic assisted vaginal hysterectomy (LAVH), and total laparoscopic hysterectomy (TLH) including both conventional and robotically assisted. Patients were then stratified according to BMI.</p><p><strong>Results: </strong>7199 records were included in the study. TLH was the most commonly performed route of hysterectomy regardless of BMI, with proportions of 50.9%, 48.9%, 50.4%, and 51.2% in ideal, overweight, obese, and morbidly obese patients, respectively. The median operative time for TAH was 2.2 hours compared to 2.7 hours for TLH (<i>p</i> < 0.01). The median length of stay for TAH was 3 days compared to 1 day for TLH (<i>p</i> < 0.01). The percentage of patients with an adverse outcome (composite indicator including transfusion, deep venous thrombosis, and infection) was 17.1 versus 3.7 for TAH and TLH, respectively (<i>p</i> < 0.01).</p><p><strong>Conclusion: </strong>During the last decade, TLH has been increasingly performed in women with uterine cancer. The increased adoption of TLH was seen in all BMI subgroups.</p>\",\"PeriodicalId\":45110,\"journal\":{\"name\":\"Minimally Invasive Surgery\",\"volume\":\"2018 \",\"pages\":\"5130856\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2018-06-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1155/2018/5130856\",\"citationCount\":\"12\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Minimally Invasive Surgery\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2018/5130856\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2018/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Minimally Invasive Surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2018/5130856","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2018/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
Association between Obesity, Surgical Route, and Perioperative Outcomes in Patients with Uterine Cancer.
Objective: To study temporal trends of hysterectomy routes performed for uterine cancer and their associations with body mass index (BMI) and perioperative morbidity.
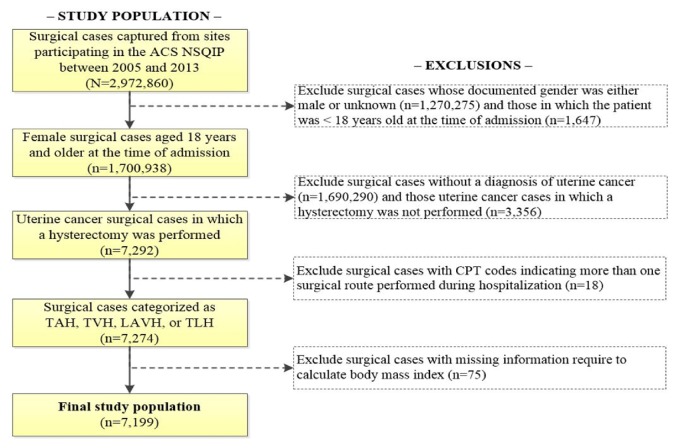
Methods: A retrospective review of the American College of Surgeons-National Surgical Quality Improvement Program (ACS-NSQIP) 2005-2013 databases was conducted. All patients who were 18 years old and older with a diagnosis of uterine cancer and underwent hysterectomy were identified using ICD-9-CM and CPT codes. Surgical route was classified into four groups: total abdominal hysterectomy (TAH), total vaginal hysterectomy (TVH), laparoscopic assisted vaginal hysterectomy (LAVH), and total laparoscopic hysterectomy (TLH) including both conventional and robotically assisted. Patients were then stratified according to BMI.
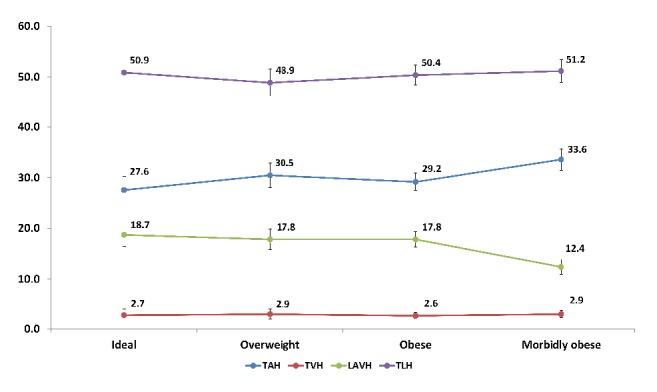
Results: 7199 records were included in the study. TLH was the most commonly performed route of hysterectomy regardless of BMI, with proportions of 50.9%, 48.9%, 50.4%, and 51.2% in ideal, overweight, obese, and morbidly obese patients, respectively. The median operative time for TAH was 2.2 hours compared to 2.7 hours for TLH (p < 0.01). The median length of stay for TAH was 3 days compared to 1 day for TLH (p < 0.01). The percentage of patients with an adverse outcome (composite indicator including transfusion, deep venous thrombosis, and infection) was 17.1 versus 3.7 for TAH and TLH, respectively (p < 0.01).
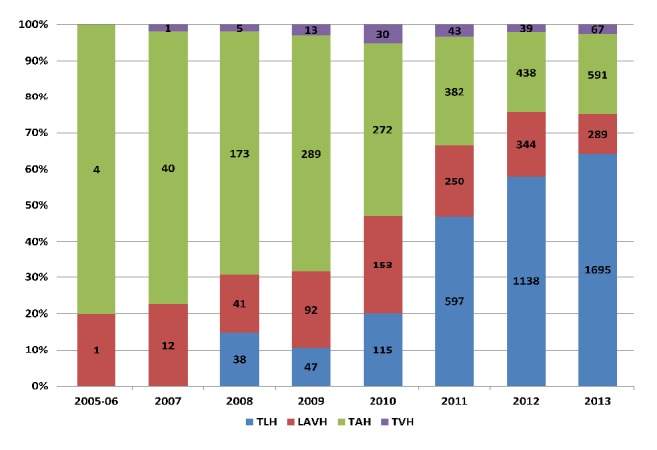
Conclusion: During the last decade, TLH has been increasingly performed in women with uterine cancer. The increased adoption of TLH was seen in all BMI subgroups.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


