Raja A Cholan, Nicole G Weiskopf, Doug Rhoton, Bhavaya Sachdeva, Nicholas V Colin, Shelby J Martin, David A Dorr
{"title":"从概念和代码到医疗保健质量测量:理解他汀类药物治疗临床质量测量值集词汇的变化。","authors":"Raja A Cholan, Nicole G Weiskopf, Doug Rhoton, Bhavaya Sachdeva, Nicholas V Colin, Shelby J Martin, David A Dorr","doi":"10.5334/egems.212","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To understand the impact of distinct concept to value set mapping on the measurement of quality of care.</p><p><strong>Background: </strong>Clinical quality measures (CQMs) intend to measure the quality of healthcare services provided, and to help promote evidence-based therapies. Most CQMs consist of grouped codes from vocabularies - or 'value sets' - that represent the unique identifiers (i.e., object identifiers), concepts (i.e., value set names), and concept definitions (i.e., code groups) that define a measure's specifications. In the development of a statin therapy CQM, two unique value sets were created by independent measure developers for the same global concepts.</p><p><strong>Methods: </strong>We first identified differences between the two value set specifications of the same CQM. We then implemented the various versions in a quality measure calculation registry to understand how the differences affected calculated prevalence of risk and measure performance.</p><p><strong>Results: </strong>Global performance rates only differed by 0.8%, but there were up to 2.3 times as many patients included with key conditions, and differing performance rates of 7.5% for patients with 'myocardial infarction' and 3.5% for those with 'ischemic vascular disease'.</p><p><strong>Conclusion: </strong>The decisions CQM developers make about which concepts and code groups to include or exclude in value set vocabularies can lead to inaccuracies in the measurement of quality of care. One solution is that developers could provide rationale for these decisions. Endorsements are needed to encourage system vendors, payers, informaticians, and clinicians to collaborate in the creation of more integrated terminology sets.</p>","PeriodicalId":72880,"journal":{"name":"EGEMS (Washington, DC)","volume":"5 1","pages":"19"},"PeriodicalIF":0.0000,"publicationDate":"2017-09-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/3c/4b/egems-5-1-212.PMC5983064.pdf","citationCount":"3","resultStr":"{\"title\":\"From Concepts and Codes to Healthcare Quality Measurement: Understanding Variations in Value Set Vocabularies for a Statin Therapy Clinical Quality Measure.\",\"authors\":\"Raja A Cholan, Nicole G Weiskopf, Doug Rhoton, Bhavaya Sachdeva, Nicholas V Colin, Shelby J Martin, David A Dorr\",\"doi\":\"10.5334/egems.212\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>To understand the impact of distinct concept to value set mapping on the measurement of quality of care.</p><p><strong>Background: </strong>Clinical quality measures (CQMs) intend to measure the quality of healthcare services provided, and to help promote evidence-based therapies. Most CQMs consist of grouped codes from vocabularies - or 'value sets' - that represent the unique identifiers (i.e., object identifiers), concepts (i.e., value set names), and concept definitions (i.e., code groups) that define a measure's specifications. In the development of a statin therapy CQM, two unique value sets were created by independent measure developers for the same global concepts.</p><p><strong>Methods: </strong>We first identified differences between the two value set specifications of the same CQM. We then implemented the various versions in a quality measure calculation registry to understand how the differences affected calculated prevalence of risk and measure performance.</p><p><strong>Results: </strong>Global performance rates only differed by 0.8%, but there were up to 2.3 times as many patients included with key conditions, and differing performance rates of 7.5% for patients with 'myocardial infarction' and 3.5% for those with 'ischemic vascular disease'.</p><p><strong>Conclusion: </strong>The decisions CQM developers make about which concepts and code groups to include or exclude in value set vocabularies can lead to inaccuracies in the measurement of quality of care. One solution is that developers could provide rationale for these decisions. Endorsements are needed to encourage system vendors, payers, informaticians, and clinicians to collaborate in the creation of more integrated terminology sets.</p>\",\"PeriodicalId\":72880,\"journal\":{\"name\":\"EGEMS (Washington, DC)\",\"volume\":\"5 1\",\"pages\":\"19\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2017-09-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/3c/4b/egems-5-1-212.PMC5983064.pdf\",\"citationCount\":\"3\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"EGEMS (Washington, DC)\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5334/egems.212\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"EGEMS (Washington, DC)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5334/egems.212","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
From Concepts and Codes to Healthcare Quality Measurement: Understanding Variations in Value Set Vocabularies for a Statin Therapy Clinical Quality Measure.
Objective: To understand the impact of distinct concept to value set mapping on the measurement of quality of care.
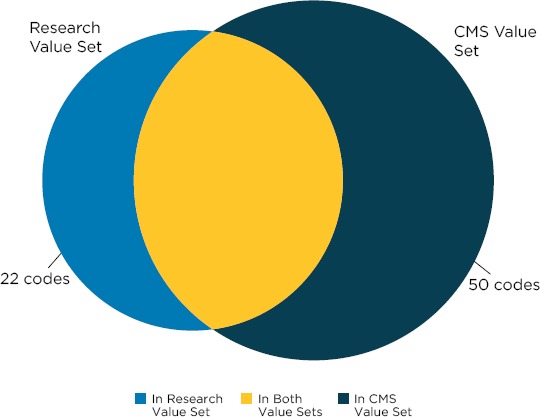
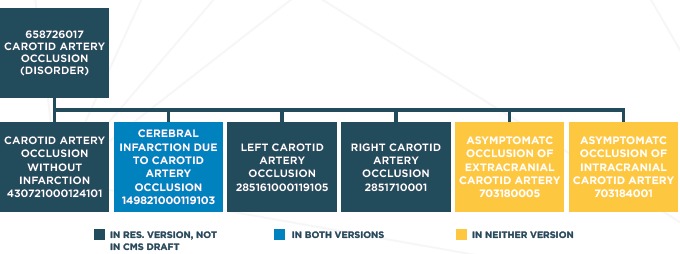
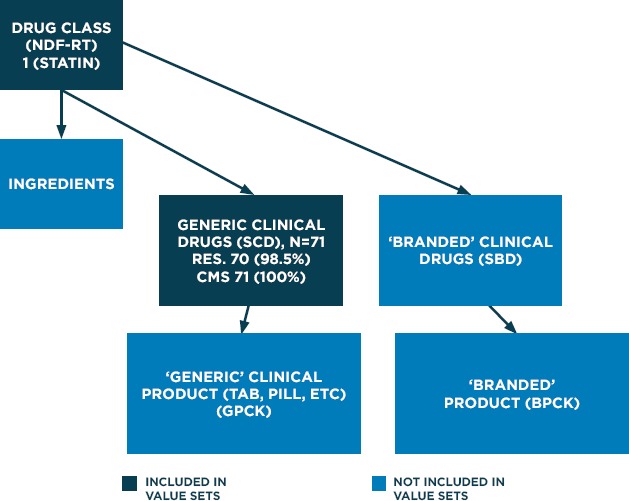
Background: Clinical quality measures (CQMs) intend to measure the quality of healthcare services provided, and to help promote evidence-based therapies. Most CQMs consist of grouped codes from vocabularies - or 'value sets' - that represent the unique identifiers (i.e., object identifiers), concepts (i.e., value set names), and concept definitions (i.e., code groups) that define a measure's specifications. In the development of a statin therapy CQM, two unique value sets were created by independent measure developers for the same global concepts.
Methods: We first identified differences between the two value set specifications of the same CQM. We then implemented the various versions in a quality measure calculation registry to understand how the differences affected calculated prevalence of risk and measure performance.
Results: Global performance rates only differed by 0.8%, but there were up to 2.3 times as many patients included with key conditions, and differing performance rates of 7.5% for patients with 'myocardial infarction' and 3.5% for those with 'ischemic vascular disease'.
Conclusion: The decisions CQM developers make about which concepts and code groups to include or exclude in value set vocabularies can lead to inaccuracies in the measurement of quality of care. One solution is that developers could provide rationale for these decisions. Endorsements are needed to encourage system vendors, payers, informaticians, and clinicians to collaborate in the creation of more integrated terminology sets.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


