Katharine H McVeigh, Elizabeth Lurie-Moroni, Pui Ying Chan, Remle Newton-Dame, Lauren Schreibstein, Kathleen S Tatem, Matthew L Romo, Lorna E Thorpe, Sharon E Perlman
{"title":"纽约市宏观电子病历监控系统指标对基于其他电子病历平台系统的推广。","authors":"Katharine H McVeigh, Elizabeth Lurie-Moroni, Pui Ying Chan, Remle Newton-Dame, Lauren Schreibstein, Kathleen S Tatem, Matthew L Romo, Lorna E Thorpe, Sharon E Perlman","doi":"10.5334/egems.247","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The New York City (NYC) Macroscope is an electronic health record (EHR) surveillance system based on a distributed network of primary care records from the Hub Population Health System. In a previous 3-part series published in <i>eGEMS</i>, we reported the validity of health indicators from the NYC Macroscope; however, questions remained regarding their generalizability to other EHR surveillance systems.</p><p><strong>Methods: </strong>We abstracted primary care chart data from more than 20 EHR software systems for 142 participants of the 2013-14 NYC Health and Nutrition Examination Survey who did not contribute data to the NYC Macroscope. We then computed the sensitivity and specificity for indicators, comparing data abstracted from EHRs with survey data.</p><p><strong>Results: </strong>Obesity and diabetes indicators had moderate to high sensitivity (0.81-0.96) and high specificity (0.94-0.98). Smoking status and hypertension indicators had moderate sensitivity (0.78-0.90) and moderate to high specificity (0.88-0.98); sensitivity improved when the sample was restricted to records from providers who attested to Stage 1 Meaningful Use. Hyperlipidemia indicators had moderate sensitivity (≥0.72) and low specificity (≤0.59), with minimal changes when restricting to Stage 1 Meaningful Use.</p><p><strong>Discussion: </strong>Indicators for obesity and diabetes used in the NYC Macroscope can be adapted to other EHR surveillance systems with minimal validation. However, additional validation of smoking status and hypertension indicators is recommended and further development of hyperlipidemia indicators is needed.</p><p><strong>Conclusion: </strong>Our findings suggest that many of the EHR-based surveillance indicators developed and validated for the NYC Macroscope are generalizable for use in other EHR surveillance systems.</p>","PeriodicalId":72880,"journal":{"name":"EGEMS (Washington, DC)","volume":"5 1","pages":"25"},"PeriodicalIF":0.0000,"publicationDate":"2017-12-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/cd/b3/egems-5-1-247.PMC5982844.pdf","citationCount":"7","resultStr":"{\"title\":\"Generalizability of Indicators from the New York City Macroscope Electronic Health Record Surveillance System to Systems Based on Other EHR Platforms.\",\"authors\":\"Katharine H McVeigh, Elizabeth Lurie-Moroni, Pui Ying Chan, Remle Newton-Dame, Lauren Schreibstein, Kathleen S Tatem, Matthew L Romo, Lorna E Thorpe, Sharon E Perlman\",\"doi\":\"10.5334/egems.247\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>The New York City (NYC) Macroscope is an electronic health record (EHR) surveillance system based on a distributed network of primary care records from the Hub Population Health System. In a previous 3-part series published in <i>eGEMS</i>, we reported the validity of health indicators from the NYC Macroscope; however, questions remained regarding their generalizability to other EHR surveillance systems.</p><p><strong>Methods: </strong>We abstracted primary care chart data from more than 20 EHR software systems for 142 participants of the 2013-14 NYC Health and Nutrition Examination Survey who did not contribute data to the NYC Macroscope. We then computed the sensitivity and specificity for indicators, comparing data abstracted from EHRs with survey data.</p><p><strong>Results: </strong>Obesity and diabetes indicators had moderate to high sensitivity (0.81-0.96) and high specificity (0.94-0.98). Smoking status and hypertension indicators had moderate sensitivity (0.78-0.90) and moderate to high specificity (0.88-0.98); sensitivity improved when the sample was restricted to records from providers who attested to Stage 1 Meaningful Use. Hyperlipidemia indicators had moderate sensitivity (≥0.72) and low specificity (≤0.59), with minimal changes when restricting to Stage 1 Meaningful Use.</p><p><strong>Discussion: </strong>Indicators for obesity and diabetes used in the NYC Macroscope can be adapted to other EHR surveillance systems with minimal validation. However, additional validation of smoking status and hypertension indicators is recommended and further development of hyperlipidemia indicators is needed.</p><p><strong>Conclusion: </strong>Our findings suggest that many of the EHR-based surveillance indicators developed and validated for the NYC Macroscope are generalizable for use in other EHR surveillance systems.</p>\",\"PeriodicalId\":72880,\"journal\":{\"name\":\"EGEMS (Washington, DC)\",\"volume\":\"5 1\",\"pages\":\"25\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2017-12-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/cd/b3/egems-5-1-247.PMC5982844.pdf\",\"citationCount\":\"7\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"EGEMS (Washington, DC)\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5334/egems.247\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"EGEMS (Washington, DC)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5334/egems.247","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Generalizability of Indicators from the New York City Macroscope Electronic Health Record Surveillance System to Systems Based on Other EHR Platforms.
Introduction: The New York City (NYC) Macroscope is an electronic health record (EHR) surveillance system based on a distributed network of primary care records from the Hub Population Health System. In a previous 3-part series published in eGEMS, we reported the validity of health indicators from the NYC Macroscope; however, questions remained regarding their generalizability to other EHR surveillance systems.
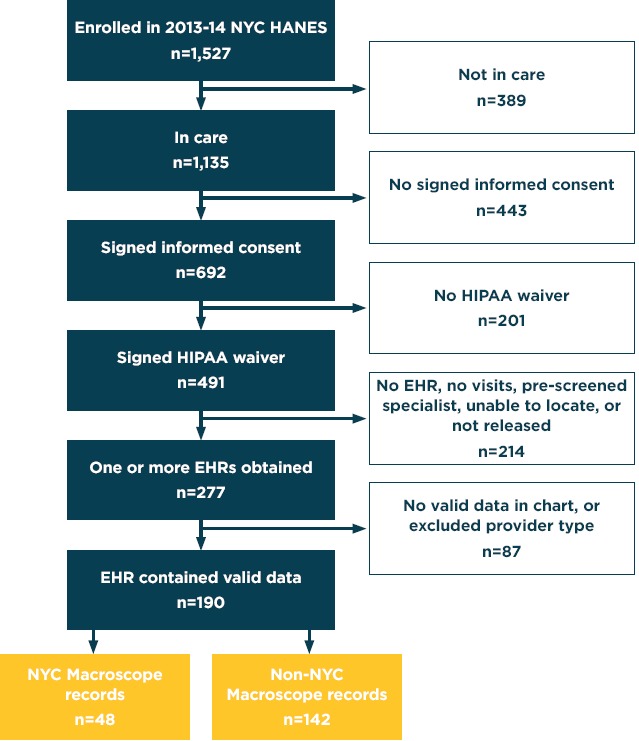
Methods: We abstracted primary care chart data from more than 20 EHR software systems for 142 participants of the 2013-14 NYC Health and Nutrition Examination Survey who did not contribute data to the NYC Macroscope. We then computed the sensitivity and specificity for indicators, comparing data abstracted from EHRs with survey data.
Results: Obesity and diabetes indicators had moderate to high sensitivity (0.81-0.96) and high specificity (0.94-0.98). Smoking status and hypertension indicators had moderate sensitivity (0.78-0.90) and moderate to high specificity (0.88-0.98); sensitivity improved when the sample was restricted to records from providers who attested to Stage 1 Meaningful Use. Hyperlipidemia indicators had moderate sensitivity (≥0.72) and low specificity (≤0.59), with minimal changes when restricting to Stage 1 Meaningful Use.
Discussion: Indicators for obesity and diabetes used in the NYC Macroscope can be adapted to other EHR surveillance systems with minimal validation. However, additional validation of smoking status and hypertension indicators is recommended and further development of hyperlipidemia indicators is needed.
Conclusion: Our findings suggest that many of the EHR-based surveillance indicators developed and validated for the NYC Macroscope are generalizable for use in other EHR surveillance systems.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


