Lara Farhat, Jasmeen Dara, Susan Duberstein, Aliva De
{"title":"利妥昔单抗治疗神经脊髓炎后的继发性低丙种球蛋白血症:病例报告。","authors":"Lara Farhat, Jasmeen Dara, Susan Duberstein, Aliva De","doi":"10.1007/s40800-018-0087-y","DOIUrl":null,"url":null,"abstract":"<p><p>A 17-year-old male with history of neuromyelitis optica and seizures presented to the pulmonology clinic for evaluation of recurrent pneumonias. He had received rituximab for the past 6 years. Over the past 2 years, he experienced four episodes of pneumonia. In between these episodes, he would improve briefly but continued to have daily cough that was productive with yellow phlegm. He also had recurrent rhinitis and sinusitis despite multiple antibiotic courses. Review of chest X-rays revealed localized right middle lobe and right lower lobe infiltrates. An extensive workup was performed, including computed tomography (CT) of the chest and bronchoscopy to rule out congenital lesions of the right lung and foreign body aspiration. Chest CT showed right lower lobe bronchiectasis. Flexible bronchoscopy with bronchoalveolar lavage showed normal anatomy with thick mucus secretions in the right lower lobe. Immunologic evaluation was performed and revealed low levels of immunoglobulin (Ig)-G, IgM, and IgA, which had declined since initiation of rituximab. Lymphocyte subset testing was remarkable for low cluster of differentiation (CD)-19. He was referred to allergy and immunology and was initiated on immunoglobulin-replacement therapy (IGRT) for acquired hypogammaglobulinemia secondary to rituximab. There was marked clinical improvement after initiation of IGRT.</p>","PeriodicalId":11364,"journal":{"name":"Drug Safety - Case Reports","volume":"5 1","pages":"22"},"PeriodicalIF":0.0000,"publicationDate":"2018-05-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/e6/c3/40800_2018_Article_87.PMC5948191.pdf","citationCount":"0","resultStr":"{\"title\":\"Secondary Hypogammaglobulinemia After Rituximab for Neuromyelitis Optica: A Case Report.\",\"authors\":\"Lara Farhat, Jasmeen Dara, Susan Duberstein, Aliva De\",\"doi\":\"10.1007/s40800-018-0087-y\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>A 17-year-old male with history of neuromyelitis optica and seizures presented to the pulmonology clinic for evaluation of recurrent pneumonias. He had received rituximab for the past 6 years. Over the past 2 years, he experienced four episodes of pneumonia. In between these episodes, he would improve briefly but continued to have daily cough that was productive with yellow phlegm. He also had recurrent rhinitis and sinusitis despite multiple antibiotic courses. Review of chest X-rays revealed localized right middle lobe and right lower lobe infiltrates. An extensive workup was performed, including computed tomography (CT) of the chest and bronchoscopy to rule out congenital lesions of the right lung and foreign body aspiration. Chest CT showed right lower lobe bronchiectasis. Flexible bronchoscopy with bronchoalveolar lavage showed normal anatomy with thick mucus secretions in the right lower lobe. Immunologic evaluation was performed and revealed low levels of immunoglobulin (Ig)-G, IgM, and IgA, which had declined since initiation of rituximab. Lymphocyte subset testing was remarkable for low cluster of differentiation (CD)-19. He was referred to allergy and immunology and was initiated on immunoglobulin-replacement therapy (IGRT) for acquired hypogammaglobulinemia secondary to rituximab. There was marked clinical improvement after initiation of IGRT.</p>\",\"PeriodicalId\":11364,\"journal\":{\"name\":\"Drug Safety - Case Reports\",\"volume\":\"5 1\",\"pages\":\"22\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2018-05-11\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/e6/c3/40800_2018_Article_87.PMC5948191.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Drug Safety - Case Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1007/s40800-018-0087-y\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Drug Safety - Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s40800-018-0087-y","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
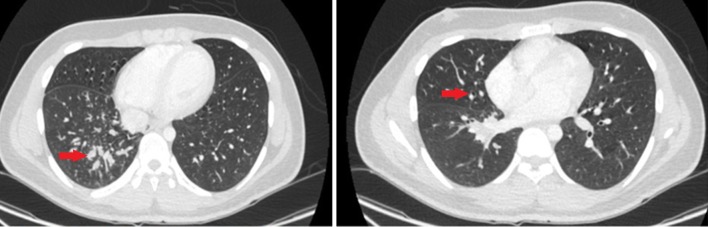
一名有神经脊髓炎视网膜病变和癫痫发作病史的 17 岁男性因反复肺炎到肺科门诊就诊。过去 6 年来,他一直在接受利妥昔单抗治疗。在过去两年中,他经历了四次肺炎发作。在这四次肺炎发作之间,他的病情会有短暂好转,但每天仍咳嗽不止,并伴有黄色痰液。尽管使用了多个抗生素疗程,他还是反复出现鼻炎和鼻窦炎。胸部 X 光片显示他的右中叶和右下叶局部浸润。为排除右肺先天性病变和异物吸入,医生进行了大量检查,包括胸部计算机断层扫描(CT)和支气管镜检查。胸部 CT 显示患者右肺下叶支气管扩张。灵活支气管镜检查和支气管肺泡灌洗显示解剖结构正常,右下叶有粘稠的粘液分泌物。免疫学评估显示,免疫球蛋白 (Ig)-G、IgM 和 IgA 水平较低,且自开始使用利妥昔单抗后有所下降。淋巴细胞亚群检测显示分化群(CD)-19偏低。他被转诊至过敏与免疫科,并开始接受免疫球蛋白替代疗法(IGRT),以治疗继发于利妥昔单抗的获得性低丙种球蛋白血症。开始 IGRT 治疗后,临床症状明显好转。
Secondary Hypogammaglobulinemia After Rituximab for Neuromyelitis Optica: A Case Report.
A 17-year-old male with history of neuromyelitis optica and seizures presented to the pulmonology clinic for evaluation of recurrent pneumonias. He had received rituximab for the past 6 years. Over the past 2 years, he experienced four episodes of pneumonia. In between these episodes, he would improve briefly but continued to have daily cough that was productive with yellow phlegm. He also had recurrent rhinitis and sinusitis despite multiple antibiotic courses. Review of chest X-rays revealed localized right middle lobe and right lower lobe infiltrates. An extensive workup was performed, including computed tomography (CT) of the chest and bronchoscopy to rule out congenital lesions of the right lung and foreign body aspiration. Chest CT showed right lower lobe bronchiectasis. Flexible bronchoscopy with bronchoalveolar lavage showed normal anatomy with thick mucus secretions in the right lower lobe. Immunologic evaluation was performed and revealed low levels of immunoglobulin (Ig)-G, IgM, and IgA, which had declined since initiation of rituximab. Lymphocyte subset testing was remarkable for low cluster of differentiation (CD)-19. He was referred to allergy and immunology and was initiated on immunoglobulin-replacement therapy (IGRT) for acquired hypogammaglobulinemia secondary to rituximab. There was marked clinical improvement after initiation of IGRT.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


