{"title":"去氨加压素诱发的严重低钠血症伴中央脑桥髓鞘溶解1例。","authors":"Tanzib Hossain, Marya Ghazipura, Vineet Reddy, Pedro J Rivera, Vikramjit Mukherjee","doi":"10.1007/s40800-018-0084-1","DOIUrl":null,"url":null,"abstract":"<p><p>Desmopressin, a synthetic vasopressin analog, is used to treat central diabetes insipidus, hemostatic disorders such as von Willebrand's disease, and nocturnal enuresis. We present the case of a 69-year-old man who developed severe hyponatremia during treatment with intranasal desmopressin at 10 µg twice daily for chronic polyuria and nocturia thought to be due to central diabetes insipidus. After 5 months of therapy, the patient noticed progressive fatigue, anorexia, dizziness, weakness, light-headedness, decreased concentration, and new-onset falls. At 6 months of therapy, the patient was brought to the emergency department for altered mental status and was found to be severely hyponatremic with a serum sodium level of 96 mmol/L, down from a value of 134 mmol/L at the initiation of therapy. The intranasal desmopressin was discontinued and the patient was admitted to the intensive care unit where the hyponatremia was slowly corrected over the next week to 132 mmol/L, never increasing by more than 8 mmol/L a day, with careful fluid management. This included infusion of over 11 L of 5% dextrose to account for a high urine output, which peaked at 7.4 L in 1 day. However, while the recommended rate for sodium correction was followed, the patient's magnetic resonance imaging of the brain obtained after discharge displayed evidence of central pontine myelinolysis. Despite this finding, the patient eventually returned to his baseline mental status with no permanent neurologic deficits.</p>","PeriodicalId":11364,"journal":{"name":"Drug Safety - Case Reports","volume":"5 1","pages":"19"},"PeriodicalIF":0.0000,"publicationDate":"2018-04-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1007/s40800-018-0084-1","citationCount":"6","resultStr":"{\"title\":\"Desmopressin-Induced Severe Hyponatremia with Central Pontine Myelinolysis: A Case Report.\",\"authors\":\"Tanzib Hossain, Marya Ghazipura, Vineet Reddy, Pedro J Rivera, Vikramjit Mukherjee\",\"doi\":\"10.1007/s40800-018-0084-1\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Desmopressin, a synthetic vasopressin analog, is used to treat central diabetes insipidus, hemostatic disorders such as von Willebrand's disease, and nocturnal enuresis. We present the case of a 69-year-old man who developed severe hyponatremia during treatment with intranasal desmopressin at 10 µg twice daily for chronic polyuria and nocturia thought to be due to central diabetes insipidus. After 5 months of therapy, the patient noticed progressive fatigue, anorexia, dizziness, weakness, light-headedness, decreased concentration, and new-onset falls. At 6 months of therapy, the patient was brought to the emergency department for altered mental status and was found to be severely hyponatremic with a serum sodium level of 96 mmol/L, down from a value of 134 mmol/L at the initiation of therapy. The intranasal desmopressin was discontinued and the patient was admitted to the intensive care unit where the hyponatremia was slowly corrected over the next week to 132 mmol/L, never increasing by more than 8 mmol/L a day, with careful fluid management. This included infusion of over 11 L of 5% dextrose to account for a high urine output, which peaked at 7.4 L in 1 day. However, while the recommended rate for sodium correction was followed, the patient's magnetic resonance imaging of the brain obtained after discharge displayed evidence of central pontine myelinolysis. Despite this finding, the patient eventually returned to his baseline mental status with no permanent neurologic deficits.</p>\",\"PeriodicalId\":11364,\"journal\":{\"name\":\"Drug Safety - Case Reports\",\"volume\":\"5 1\",\"pages\":\"19\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2018-04-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1007/s40800-018-0084-1\",\"citationCount\":\"6\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Drug Safety - Case Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1007/s40800-018-0084-1\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Drug Safety - Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s40800-018-0084-1","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Desmopressin-Induced Severe Hyponatremia with Central Pontine Myelinolysis: A Case Report.
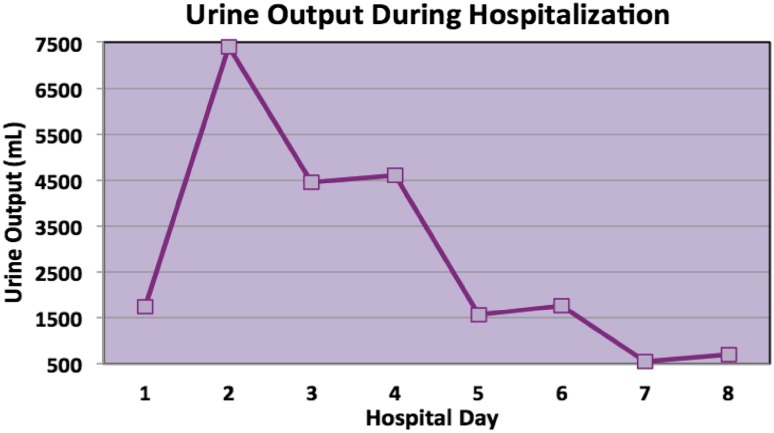
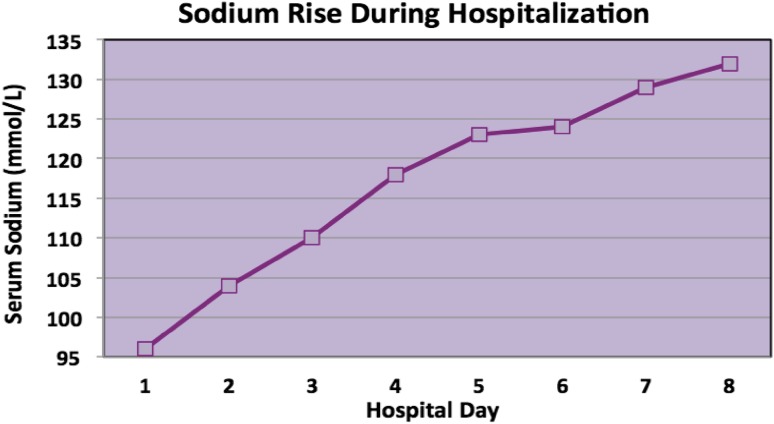
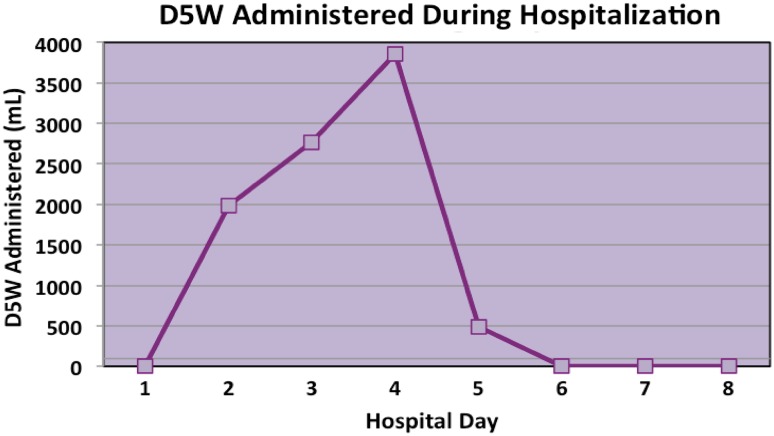
Desmopressin, a synthetic vasopressin analog, is used to treat central diabetes insipidus, hemostatic disorders such as von Willebrand's disease, and nocturnal enuresis. We present the case of a 69-year-old man who developed severe hyponatremia during treatment with intranasal desmopressin at 10 µg twice daily for chronic polyuria and nocturia thought to be due to central diabetes insipidus. After 5 months of therapy, the patient noticed progressive fatigue, anorexia, dizziness, weakness, light-headedness, decreased concentration, and new-onset falls. At 6 months of therapy, the patient was brought to the emergency department for altered mental status and was found to be severely hyponatremic with a serum sodium level of 96 mmol/L, down from a value of 134 mmol/L at the initiation of therapy. The intranasal desmopressin was discontinued and the patient was admitted to the intensive care unit where the hyponatremia was slowly corrected over the next week to 132 mmol/L, never increasing by more than 8 mmol/L a day, with careful fluid management. This included infusion of over 11 L of 5% dextrose to account for a high urine output, which peaked at 7.4 L in 1 day. However, while the recommended rate for sodium correction was followed, the patient's magnetic resonance imaging of the brain obtained after discharge displayed evidence of central pontine myelinolysis. Despite this finding, the patient eventually returned to his baseline mental status with no permanent neurologic deficits.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


