{"title":"头孢唑林相关性急性间质性肾炎伴肾范围蛋白尿1例报告。","authors":"Ang Xu, David Hyman, Lee Bach Lu","doi":"10.1007/s40800-018-0080-5","DOIUrl":null,"url":null,"abstract":"<p><p>A 67-year-old male with history of well controlled type 2 diabetes mellitus and hypertension developed acute interstitial nephritis (AIN) with nephrotic-range proteinuria during treatment with cefazolin for methicillin-sensitive Staphylococcus aureus and Group B Streptococcus (GBS) bacteremia. The patient received intravenous cefazolin 2 g every 8 h for 4 weeks prior to presentation to the emergency department with abdominal distension, nausea, and vomiting. Investigations revealed a serum ascites albumin gradient of 1.0 with total protein of 1.8 g/dL suggestive of nephrotic syndrome, which was confirmed with a spot urine protein/creatinine ratio that estimated 7.95 g of protein per day. Serum creatinine was elevated compared with baseline. Urine studies showed sterile pyuria with 3+ protein and eosinophiluria. The patient was diagnosed with AIN with nephrotic-range proteinuria associated with cefazolin use. Cefazolin was discontinued and, within a couple of days, the patient's creatinine stabilized. He was discharged with prednisone 60 mg once a day for 10 days with a taper over 2 weeks for his AIN. The patient's creatinine and proteinuria slowly decreased over the next couple of weeks, however, did not recover to baseline. A Naranjo assessment score of 6 was obtained, indicating a probable relationship between the patient's AIN with nephrotic-range proteinuria and his use of cefazolin.</p>","PeriodicalId":11364,"journal":{"name":"Drug Safety - Case Reports","volume":"5 1","pages":"16"},"PeriodicalIF":0.0000,"publicationDate":"2018-04-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1007/s40800-018-0080-5","citationCount":"1","resultStr":"{\"title\":\"Cefazolin-Related Acute Interstitial Nephritis with Associated Nephrotic-Range Proteinuria: A Case Report.\",\"authors\":\"Ang Xu, David Hyman, Lee Bach Lu\",\"doi\":\"10.1007/s40800-018-0080-5\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>A 67-year-old male with history of well controlled type 2 diabetes mellitus and hypertension developed acute interstitial nephritis (AIN) with nephrotic-range proteinuria during treatment with cefazolin for methicillin-sensitive Staphylococcus aureus and Group B Streptococcus (GBS) bacteremia. The patient received intravenous cefazolin 2 g every 8 h for 4 weeks prior to presentation to the emergency department with abdominal distension, nausea, and vomiting. Investigations revealed a serum ascites albumin gradient of 1.0 with total protein of 1.8 g/dL suggestive of nephrotic syndrome, which was confirmed with a spot urine protein/creatinine ratio that estimated 7.95 g of protein per day. Serum creatinine was elevated compared with baseline. Urine studies showed sterile pyuria with 3+ protein and eosinophiluria. The patient was diagnosed with AIN with nephrotic-range proteinuria associated with cefazolin use. Cefazolin was discontinued and, within a couple of days, the patient's creatinine stabilized. He was discharged with prednisone 60 mg once a day for 10 days with a taper over 2 weeks for his AIN. The patient's creatinine and proteinuria slowly decreased over the next couple of weeks, however, did not recover to baseline. A Naranjo assessment score of 6 was obtained, indicating a probable relationship between the patient's AIN with nephrotic-range proteinuria and his use of cefazolin.</p>\",\"PeriodicalId\":11364,\"journal\":{\"name\":\"Drug Safety - Case Reports\",\"volume\":\"5 1\",\"pages\":\"16\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2018-04-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1007/s40800-018-0080-5\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Drug Safety - Case Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1007/s40800-018-0080-5\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Drug Safety - Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s40800-018-0080-5","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Cefazolin-Related Acute Interstitial Nephritis with Associated Nephrotic-Range Proteinuria: A Case Report.
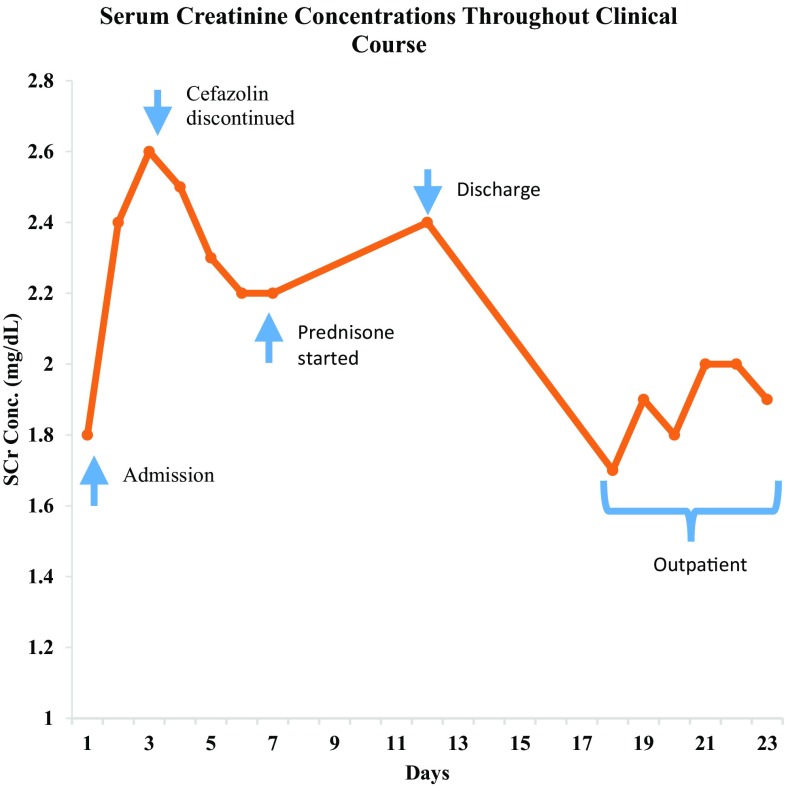
A 67-year-old male with history of well controlled type 2 diabetes mellitus and hypertension developed acute interstitial nephritis (AIN) with nephrotic-range proteinuria during treatment with cefazolin for methicillin-sensitive Staphylococcus aureus and Group B Streptococcus (GBS) bacteremia. The patient received intravenous cefazolin 2 g every 8 h for 4 weeks prior to presentation to the emergency department with abdominal distension, nausea, and vomiting. Investigations revealed a serum ascites albumin gradient of 1.0 with total protein of 1.8 g/dL suggestive of nephrotic syndrome, which was confirmed with a spot urine protein/creatinine ratio that estimated 7.95 g of protein per day. Serum creatinine was elevated compared with baseline. Urine studies showed sterile pyuria with 3+ protein and eosinophiluria. The patient was diagnosed with AIN with nephrotic-range proteinuria associated with cefazolin use. Cefazolin was discontinued and, within a couple of days, the patient's creatinine stabilized. He was discharged with prednisone 60 mg once a day for 10 days with a taper over 2 weeks for his AIN. The patient's creatinine and proteinuria slowly decreased over the next couple of weeks, however, did not recover to baseline. A Naranjo assessment score of 6 was obtained, indicating a probable relationship between the patient's AIN with nephrotic-range proteinuria and his use of cefazolin.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


