Jacqueline N Poston, Russell Dorer, David M Aboulafia
{"title":"潜水钟和蝴蝶重访:一名患有爱泼斯坦-巴尔病毒阳性弥漫性大b细胞淋巴瘤的男子闭锁综合征的致命病例,没有其他说明。","authors":"Jacqueline N Poston, Russell Dorer, David M Aboulafia","doi":"10.1177/1179545X18762799","DOIUrl":null,"url":null,"abstract":"<p><p>Epstein-Barr virus (EBV)-positive diffuse large B-cell lymphoma (DLBCL) is a rare variant of DLBCL. The natural history of this subtype is poorly understood. Incomplete literature in the era of rituximab suggests that patients with EBV-positive DLBCL have similar outcomes to patients with EBV-negative DLBCL when treated with rituximab and anthracycline-based chemotherapy regimens; however, there are few prospective studies on this subtype and little is known about the risk of central nervous system (CNS) relapse with EBV-positive DLBCL. Herein, we describe the case of a 64-year-old man who presented with stage IIA EBV-positive DLBCL. His international age-adjusted International Prognostic Index (IPI) was 2. He achieved a complete response to 6 cycles of rituximab combined with chemotherapy consisting of dose-adjusted etoposide, prednisone, vincristine, cyclophosphamide, and doxorubicin. After 10 days of completion of chemotherapy, he had a fulminant neurologic decline manifested by diffuse weakness followed by a locked-in syndrome; he could only communicate by moving his eyes. He had been deemed at low risk for CNS relapse based on the application of the recently developed CNS-IPI score of 2 (1 point for age >60 years and 1 point for lactate dehydrogenase higher than normal) and consequently did not receive therapy for CNS prophylaxis. A limited postmortem autopsy revealed extensive lymphoma throughout the brain, particularly in the deep basal nuclei, midbrain, pons, centrum semiovale, and corpus callosum. This presentation of CNS relapse is rare and has not yet been described in EBV-positive DLBCL. We discuss some of the unique aspects of this case including the clinical manifestations of locked-in syndrome and its differential diagnosis and the uncertain benefits of CNS prophylaxis in this clinical context.</p>","PeriodicalId":43083,"journal":{"name":"Clinical Medicine Insights-Blood Disorders","volume":"11 ","pages":"1179545X18762799"},"PeriodicalIF":3.0000,"publicationDate":"2018-03-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1177/1179545X18762799","citationCount":"2","resultStr":"{\"title\":\"The Diving Bell and the Butterfly Revisited: A Fatal Case of Locked-in Syndrome in a Man With Epstein-Barr Virus-Positive Diffuse Large B-Cell Lymphoma, Not Otherwise Specified.\",\"authors\":\"Jacqueline N Poston, Russell Dorer, David M Aboulafia\",\"doi\":\"10.1177/1179545X18762799\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Epstein-Barr virus (EBV)-positive diffuse large B-cell lymphoma (DLBCL) is a rare variant of DLBCL. The natural history of this subtype is poorly understood. Incomplete literature in the era of rituximab suggests that patients with EBV-positive DLBCL have similar outcomes to patients with EBV-negative DLBCL when treated with rituximab and anthracycline-based chemotherapy regimens; however, there are few prospective studies on this subtype and little is known about the risk of central nervous system (CNS) relapse with EBV-positive DLBCL. Herein, we describe the case of a 64-year-old man who presented with stage IIA EBV-positive DLBCL. His international age-adjusted International Prognostic Index (IPI) was 2. He achieved a complete response to 6 cycles of rituximab combined with chemotherapy consisting of dose-adjusted etoposide, prednisone, vincristine, cyclophosphamide, and doxorubicin. After 10 days of completion of chemotherapy, he had a fulminant neurologic decline manifested by diffuse weakness followed by a locked-in syndrome; he could only communicate by moving his eyes. He had been deemed at low risk for CNS relapse based on the application of the recently developed CNS-IPI score of 2 (1 point for age >60 years and 1 point for lactate dehydrogenase higher than normal) and consequently did not receive therapy for CNS prophylaxis. A limited postmortem autopsy revealed extensive lymphoma throughout the brain, particularly in the deep basal nuclei, midbrain, pons, centrum semiovale, and corpus callosum. This presentation of CNS relapse is rare and has not yet been described in EBV-positive DLBCL. We discuss some of the unique aspects of this case including the clinical manifestations of locked-in syndrome and its differential diagnosis and the uncertain benefits of CNS prophylaxis in this clinical context.</p>\",\"PeriodicalId\":43083,\"journal\":{\"name\":\"Clinical Medicine Insights-Blood Disorders\",\"volume\":\"11 \",\"pages\":\"1179545X18762799\"},\"PeriodicalIF\":3.0000,\"publicationDate\":\"2018-03-26\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1177/1179545X18762799\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Medicine Insights-Blood Disorders\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/1179545X18762799\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2018/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine Insights-Blood Disorders","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/1179545X18762799","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2018/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
The Diving Bell and the Butterfly Revisited: A Fatal Case of Locked-in Syndrome in a Man With Epstein-Barr Virus-Positive Diffuse Large B-Cell Lymphoma, Not Otherwise Specified.
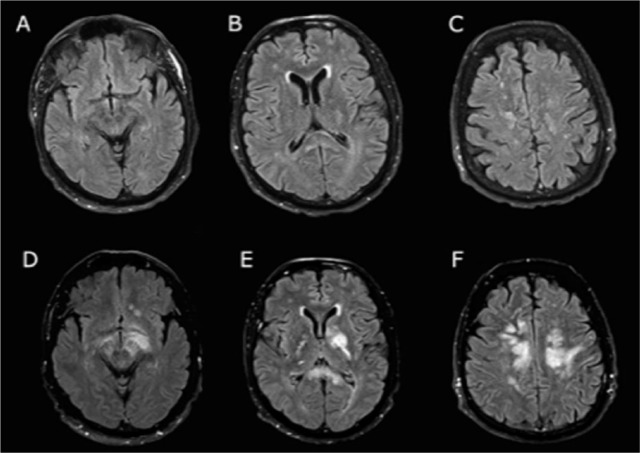
Epstein-Barr virus (EBV)-positive diffuse large B-cell lymphoma (DLBCL) is a rare variant of DLBCL. The natural history of this subtype is poorly understood. Incomplete literature in the era of rituximab suggests that patients with EBV-positive DLBCL have similar outcomes to patients with EBV-negative DLBCL when treated with rituximab and anthracycline-based chemotherapy regimens; however, there are few prospective studies on this subtype and little is known about the risk of central nervous system (CNS) relapse with EBV-positive DLBCL. Herein, we describe the case of a 64-year-old man who presented with stage IIA EBV-positive DLBCL. His international age-adjusted International Prognostic Index (IPI) was 2. He achieved a complete response to 6 cycles of rituximab combined with chemotherapy consisting of dose-adjusted etoposide, prednisone, vincristine, cyclophosphamide, and doxorubicin. After 10 days of completion of chemotherapy, he had a fulminant neurologic decline manifested by diffuse weakness followed by a locked-in syndrome; he could only communicate by moving his eyes. He had been deemed at low risk for CNS relapse based on the application of the recently developed CNS-IPI score of 2 (1 point for age >60 years and 1 point for lactate dehydrogenase higher than normal) and consequently did not receive therapy for CNS prophylaxis. A limited postmortem autopsy revealed extensive lymphoma throughout the brain, particularly in the deep basal nuclei, midbrain, pons, centrum semiovale, and corpus callosum. This presentation of CNS relapse is rare and has not yet been described in EBV-positive DLBCL. We discuss some of the unique aspects of this case including the clinical manifestations of locked-in syndrome and its differential diagnosis and the uncertain benefits of CNS prophylaxis in this clinical context.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


