Taysir S Garadah, Khalid Bin Thani, Leena Sulibech, Ahmed A Jaradat, Mohamed E Al Alawi, Haytham Amin
{"title":"巴林急性冠脉综合征(ACS)患者的风险分层和医院道德。","authors":"Taysir S Garadah, Khalid Bin Thani, Leena Sulibech, Ahmed A Jaradat, Mohamed E Al Alawi, Haytham Amin","doi":"10.2174/1874192401812010007","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Risk factors and short-term mortality in patients presented with Acute Coronary Syndrome (ACS) in Bahrain has not been evaluated before.</p><p><strong>Aim: </strong>In this prospective observational study, we aim to determine the clinical risk profiles of patients with ACS in Bahrain and describe the incidence, pattern of presentation and predictors of in-hospital clinical outcomes after admission.</p><p><strong>Methods: </strong>Patients with ACS were prospectively enrolled over a 12 month period. The rate of incidence of risk factors in patients was compared with 635 non-cardiac patient admissions that matched for age and gender. Multiple logistic regression analysis was used to predict poor outcomes in patients with ACS. The variables were ages >65 years, body mass index (BMI) >28 kg/m<sup>2</sup>, GRACE (Global Registry of Acute Coronary Events) score >170, history of diabetes mellitus (DM), systolic hypertension >180 mmHg, level of creatinine >160 μmol/l and Heart Rate (HR) on admission >90 bpm, serum troponin rise and ST segment elevation on the ECG.</p><p><strong>Results: </strong>Patients with ACS (n=635) were enrolled consecutively. Mean age was 61.3 ± 13.2 years, with 417 (65.6%) male. Mean age for patients with ST-segment elevation myocardial infarction (STEMI, n=156) compared with non-STEMI (NSTEMI, n=158) and unstable angina (UA, n=321) was 56.5± 12.8 <i>vs</i> 62.5±14.0 years respectively. In-hospital mortality was 5.1%, 3.1% and 2.5% for patients with STEMI, NSTEMI, and UA, respectively. In STEMI patients, thrombolytic therapy was performed in 88 (56.5%) patients and 68 (43.5%) had primary coronary angioplasty (PCI). The predictive value of different clinical variables for in-hospital mortality and cardiac events in the study were: 2.8 for GRACE score >170, 3.1 for DM, 2.2 for SBP >180 mmHg, 1.4 for age >65 years, 1.8 for BMI >28, 1.7 for creatinine >160 μmol/L, 2.1 for HR >90 bpm, 2.2 for positive serum troponin and 2.3 for ST elevation.</p><p><strong>Conclusion: </strong>Patients with STEMI compared with NSTEMI and UA were of younger age. There was higher in-hospital mortality in STEMI compared with NSTEMI and UA patients. The most significant predictors of death or cardiac events on admission in ACS were DM, GRACE Score >170, systolic hypertension >180 mmHg, positive serum troponin and HR >90 bpm.</p>","PeriodicalId":504447,"journal":{"name":"The Open Cardiovascular Medicine Journal","volume":"12 ","pages":"7-17"},"PeriodicalIF":0.0000,"publicationDate":"2018-02-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5838636/pdf/","citationCount":"9","resultStr":"{\"title\":\"Risk Stratification and in Hospital Morality in Patients Presenting with Acute Coronary Syndrome (ACS) in Bahrain.\",\"authors\":\"Taysir S Garadah, Khalid Bin Thani, Leena Sulibech, Ahmed A Jaradat, Mohamed E Al Alawi, Haytham Amin\",\"doi\":\"10.2174/1874192401812010007\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Risk factors and short-term mortality in patients presented with Acute Coronary Syndrome (ACS) in Bahrain has not been evaluated before.</p><p><strong>Aim: </strong>In this prospective observational study, we aim to determine the clinical risk profiles of patients with ACS in Bahrain and describe the incidence, pattern of presentation and predictors of in-hospital clinical outcomes after admission.</p><p><strong>Methods: </strong>Patients with ACS were prospectively enrolled over a 12 month period. The rate of incidence of risk factors in patients was compared with 635 non-cardiac patient admissions that matched for age and gender. Multiple logistic regression analysis was used to predict poor outcomes in patients with ACS. The variables were ages >65 years, body mass index (BMI) >28 kg/m<sup>2</sup>, GRACE (Global Registry of Acute Coronary Events) score >170, history of diabetes mellitus (DM), systolic hypertension >180 mmHg, level of creatinine >160 μmol/l and Heart Rate (HR) on admission >90 bpm, serum troponin rise and ST segment elevation on the ECG.</p><p><strong>Results: </strong>Patients with ACS (n=635) were enrolled consecutively. Mean age was 61.3 ± 13.2 years, with 417 (65.6%) male. Mean age for patients with ST-segment elevation myocardial infarction (STEMI, n=156) compared with non-STEMI (NSTEMI, n=158) and unstable angina (UA, n=321) was 56.5± 12.8 <i>vs</i> 62.5±14.0 years respectively. In-hospital mortality was 5.1%, 3.1% and 2.5% for patients with STEMI, NSTEMI, and UA, respectively. In STEMI patients, thrombolytic therapy was performed in 88 (56.5%) patients and 68 (43.5%) had primary coronary angioplasty (PCI). The predictive value of different clinical variables for in-hospital mortality and cardiac events in the study were: 2.8 for GRACE score >170, 3.1 for DM, 2.2 for SBP >180 mmHg, 1.4 for age >65 years, 1.8 for BMI >28, 1.7 for creatinine >160 μmol/L, 2.1 for HR >90 bpm, 2.2 for positive serum troponin and 2.3 for ST elevation.</p><p><strong>Conclusion: </strong>Patients with STEMI compared with NSTEMI and UA were of younger age. There was higher in-hospital mortality in STEMI compared with NSTEMI and UA patients. The most significant predictors of death or cardiac events on admission in ACS were DM, GRACE Score >170, systolic hypertension >180 mmHg, positive serum troponin and HR >90 bpm.</p>\",\"PeriodicalId\":504447,\"journal\":{\"name\":\"The Open Cardiovascular Medicine Journal\",\"volume\":\"12 \",\"pages\":\"7-17\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2018-02-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5838636/pdf/\",\"citationCount\":\"9\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"The Open Cardiovascular Medicine Journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2174/1874192401812010007\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2018/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Open Cardiovascular Medicine Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2174/1874192401812010007","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2018/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Risk Stratification and in Hospital Morality in Patients Presenting with Acute Coronary Syndrome (ACS) in Bahrain.
Background: Risk factors and short-term mortality in patients presented with Acute Coronary Syndrome (ACS) in Bahrain has not been evaluated before.
Aim: In this prospective observational study, we aim to determine the clinical risk profiles of patients with ACS in Bahrain and describe the incidence, pattern of presentation and predictors of in-hospital clinical outcomes after admission.
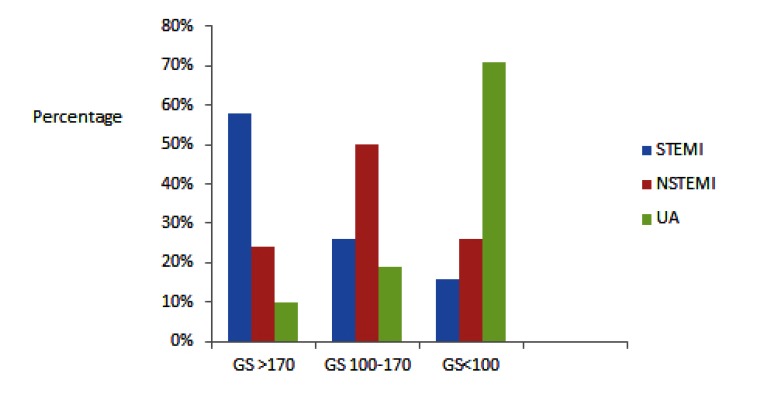
Methods: Patients with ACS were prospectively enrolled over a 12 month period. The rate of incidence of risk factors in patients was compared with 635 non-cardiac patient admissions that matched for age and gender. Multiple logistic regression analysis was used to predict poor outcomes in patients with ACS. The variables were ages >65 years, body mass index (BMI) >28 kg/m2, GRACE (Global Registry of Acute Coronary Events) score >170, history of diabetes mellitus (DM), systolic hypertension >180 mmHg, level of creatinine >160 μmol/l and Heart Rate (HR) on admission >90 bpm, serum troponin rise and ST segment elevation on the ECG.
Results: Patients with ACS (n=635) were enrolled consecutively. Mean age was 61.3 ± 13.2 years, with 417 (65.6%) male. Mean age for patients with ST-segment elevation myocardial infarction (STEMI, n=156) compared with non-STEMI (NSTEMI, n=158) and unstable angina (UA, n=321) was 56.5± 12.8 vs 62.5±14.0 years respectively. In-hospital mortality was 5.1%, 3.1% and 2.5% for patients with STEMI, NSTEMI, and UA, respectively. In STEMI patients, thrombolytic therapy was performed in 88 (56.5%) patients and 68 (43.5%) had primary coronary angioplasty (PCI). The predictive value of different clinical variables for in-hospital mortality and cardiac events in the study were: 2.8 for GRACE score >170, 3.1 for DM, 2.2 for SBP >180 mmHg, 1.4 for age >65 years, 1.8 for BMI >28, 1.7 for creatinine >160 μmol/L, 2.1 for HR >90 bpm, 2.2 for positive serum troponin and 2.3 for ST elevation.
Conclusion: Patients with STEMI compared with NSTEMI and UA were of younger age. There was higher in-hospital mortality in STEMI compared with NSTEMI and UA patients. The most significant predictors of death or cardiac events on admission in ACS were DM, GRACE Score >170, systolic hypertension >180 mmHg, positive serum troponin and HR >90 bpm.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


