Shamus O’Meagher , Madhusudan Ganigara , David J. Tanous , David S. Celermajer , Rajesh Puranik
{"title":"成人法洛四联症和游离肺反流修复后右心室扩张的进展","authors":"Shamus O’Meagher , Madhusudan Ganigara , David J. Tanous , David S. Celermajer , Rajesh Puranik","doi":"10.1016/j.ijchv.2014.02.003","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p>The time course of progressive dilatation of the right ventricle (RV) in adults with pulmonary regurgitation (PR) late after repair of tetralogy of Fallot (TOF) is poorly characterized.</p></div><div><h3>Methods</h3><p>We analysed cardiac MRI data (1.5 T) from 14 adult repaired TOF patients (26 ± 11 years of age) with dilated RVs and known significant PR, on 2 separate visits with a between MRI period of 2.1 ± 1.0 years.</p></div><div><h3>Results</h3><p>Indexed RV end diastolic volume (RVEDVi) increased over 2 years (142 ± 19 to 151 ± 20 mL/m<sup>2</sup>, <em>p</em> = 0.005; change = 8.4 ± 9.3 mL/m<sup>2</sup>, range = − 6 to 26 mL/m<sup>2</sup>; annual mL/m<sup>2</sup> increase = 4.3 ± 4.6; annual percentage increase = 3.1 ± 3.3%), whilst RV ejection fraction decreased (53 ± 8 to 49 ± 7 %, <em>p</em> = 0.039). RV muscular corpus (RVMC) EDVi significantly increased (130 ± 19 to 138 ± 20 mL/m<sup>2</sup>, <em>p</em> = 0.014), whereas RV outflow tract (RVOT) EDVi did not (12 ± 7 vs 13 ± 6 mL/m<sup>2</sup>, <em>p</em> = 0.390). No other RV or LV measures significantly changed during the inter-MRI period. The change in RVEDVi correlated significantly with LV end diastolic volume (<em>r</em> = − 0.582, <em>p</em> = 0.029), RVEDVi:LVEDVi (<em>r</em> = 0.6, <em>p</em> = 0.023) and RVMC EDVi (<em>r</em> = 0.9, <em>p</em> < 0.001) but not RVOT EDVi (<em>r</em> = 0.225, <em>p</em> = 0.459).</p></div><div><h3>Conclusions</h3><p>Adult repaired TOF patients with free PR experienced a mean 3.1%, or 4.3 mL/m<sup>2</sup>, annual increase in RVEDVi, unrelated to the initial RVEDVi or PR fraction. The increase in RVEDVi was due to RVMC rather than RVOT dilatation. This provides a guide to the frequency of MR surveillance and insights into the natural history of progressive RV dilatation in this setting.</p></div>","PeriodicalId":90542,"journal":{"name":"International journal of cardiology. Heart & vessels","volume":"3 ","pages":"Pages 28-31"},"PeriodicalIF":0.0000,"publicationDate":"2014-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1016/j.ijchv.2014.02.003","citationCount":"2","resultStr":"{\"title\":\"Progress of right ventricular dilatation in adults with repaired tetralogy of Fallot and free pulmonary regurgitation\",\"authors\":\"Shamus O’Meagher , Madhusudan Ganigara , David J. Tanous , David S. Celermajer , Rajesh Puranik\",\"doi\":\"10.1016/j.ijchv.2014.02.003\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Background</h3><p>The time course of progressive dilatation of the right ventricle (RV) in adults with pulmonary regurgitation (PR) late after repair of tetralogy of Fallot (TOF) is poorly characterized.</p></div><div><h3>Methods</h3><p>We analysed cardiac MRI data (1.5 T) from 14 adult repaired TOF patients (26 ± 11 years of age) with dilated RVs and known significant PR, on 2 separate visits with a between MRI period of 2.1 ± 1.0 years.</p></div><div><h3>Results</h3><p>Indexed RV end diastolic volume (RVEDVi) increased over 2 years (142 ± 19 to 151 ± 20 mL/m<sup>2</sup>, <em>p</em> = 0.005; change = 8.4 ± 9.3 mL/m<sup>2</sup>, range = − 6 to 26 mL/m<sup>2</sup>; annual mL/m<sup>2</sup> increase = 4.3 ± 4.6; annual percentage increase = 3.1 ± 3.3%), whilst RV ejection fraction decreased (53 ± 8 to 49 ± 7 %, <em>p</em> = 0.039). RV muscular corpus (RVMC) EDVi significantly increased (130 ± 19 to 138 ± 20 mL/m<sup>2</sup>, <em>p</em> = 0.014), whereas RV outflow tract (RVOT) EDVi did not (12 ± 7 vs 13 ± 6 mL/m<sup>2</sup>, <em>p</em> = 0.390). No other RV or LV measures significantly changed during the inter-MRI period. The change in RVEDVi correlated significantly with LV end diastolic volume (<em>r</em> = − 0.582, <em>p</em> = 0.029), RVEDVi:LVEDVi (<em>r</em> = 0.6, <em>p</em> = 0.023) and RVMC EDVi (<em>r</em> = 0.9, <em>p</em> < 0.001) but not RVOT EDVi (<em>r</em> = 0.225, <em>p</em> = 0.459).</p></div><div><h3>Conclusions</h3><p>Adult repaired TOF patients with free PR experienced a mean 3.1%, or 4.3 mL/m<sup>2</sup>, annual increase in RVEDVi, unrelated to the initial RVEDVi or PR fraction. The increase in RVEDVi was due to RVMC rather than RVOT dilatation. This provides a guide to the frequency of MR surveillance and insights into the natural history of progressive RV dilatation in this setting.</p></div>\",\"PeriodicalId\":90542,\"journal\":{\"name\":\"International journal of cardiology. Heart & vessels\",\"volume\":\"3 \",\"pages\":\"Pages 28-31\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2014-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1016/j.ijchv.2014.02.003\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International journal of cardiology. Heart & vessels\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2214763214000066\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International journal of cardiology. Heart & vessels","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2214763214000066","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 2
摘要
成人法洛四联症(TOF)修复后晚期肺反流(PR)患者右心室进行性扩张(RV)的时间过程尚不清楚。方法对14例成人修复TOF患者(26±11岁)的心脏MRI数据(1.5 T)进行分析,这些患者的RVs扩张,PR明显,MRI周期为2.1±1.0年。结果指标右心室舒张末期容积(RVEDVi)在2年内升高(142±19 ~ 151±20 mL/m2, p = 0.005;变化= 8.4±9.3 mL/m2,变化范围=−6 ~ 26 mL/m2;mL/m2年增长= 4.3±4.6;右心室射血分数下降(53±8 ~ 49±7%,p = 0.039)。右心室肌体(RVMC) EDVi显著升高(130±19 ~ 138±20 mL/m2, p = 0.014),而右心室流出道(RVOT) EDVi无显著升高(12±7 vs 13±6 mL/m2, p = 0.390)。其他RV或LV测量在mri间期无明显变化。RVEDVi变化与左室舒张末期容积(r = - 0.582, p = 0.029)、RVEDVi:LVEDVi (r = 0.6, p = 0.023)、RVMC EDVi (r = 0.9, p <0.001),但RVOT EDVi没有(r = 0.225, p = 0.459)。结论:成人游离PR修复TOF患者的RVEDVi平均每年增加3.1%,即4.3 mL/m2,与初始RVEDVi或PR分数无关。RVEDVi的增加是由于RVMC而不是RVOT扩张。这为MR监测的频率提供了指导,并对这种情况下进行性右心室扩张的自然史有了深入的了解。
Progress of right ventricular dilatation in adults with repaired tetralogy of Fallot and free pulmonary regurgitation
Background
The time course of progressive dilatation of the right ventricle (RV) in adults with pulmonary regurgitation (PR) late after repair of tetralogy of Fallot (TOF) is poorly characterized.
Methods
We analysed cardiac MRI data (1.5 T) from 14 adult repaired TOF patients (26 ± 11 years of age) with dilated RVs and known significant PR, on 2 separate visits with a between MRI period of 2.1 ± 1.0 years.
Results
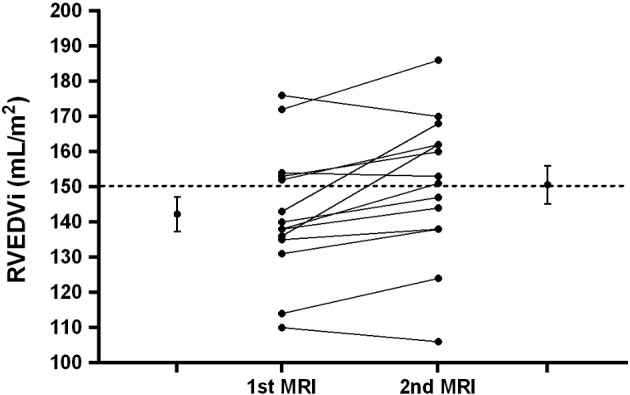
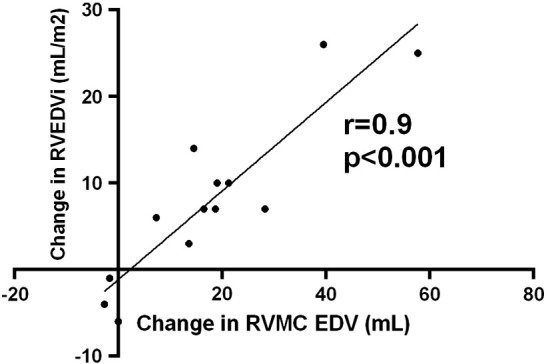
Indexed RV end diastolic volume (RVEDVi) increased over 2 years (142 ± 19 to 151 ± 20 mL/m2, p = 0.005; change = 8.4 ± 9.3 mL/m2, range = − 6 to 26 mL/m2; annual mL/m2 increase = 4.3 ± 4.6; annual percentage increase = 3.1 ± 3.3%), whilst RV ejection fraction decreased (53 ± 8 to 49 ± 7 %, p = 0.039). RV muscular corpus (RVMC) EDVi significantly increased (130 ± 19 to 138 ± 20 mL/m2, p = 0.014), whereas RV outflow tract (RVOT) EDVi did not (12 ± 7 vs 13 ± 6 mL/m2, p = 0.390). No other RV or LV measures significantly changed during the inter-MRI period. The change in RVEDVi correlated significantly with LV end diastolic volume (r = − 0.582, p = 0.029), RVEDVi:LVEDVi (r = 0.6, p = 0.023) and RVMC EDVi (r = 0.9, p < 0.001) but not RVOT EDVi (r = 0.225, p = 0.459).
Conclusions
Adult repaired TOF patients with free PR experienced a mean 3.1%, or 4.3 mL/m2, annual increase in RVEDVi, unrelated to the initial RVEDVi or PR fraction. The increase in RVEDVi was due to RVMC rather than RVOT dilatation. This provides a guide to the frequency of MR surveillance and insights into the natural history of progressive RV dilatation in this setting.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


