Rahul R Parikh, Amil Patel, Sinae Kim, Isaac Yi Kim, Sharad Goyal
{"title":"腹腔镜前列腺切除术与开放式前列腺切除术对低危前列腺癌患者的疗效比较:一项匹配病例对照研究。","authors":"Rahul R Parikh, Amil Patel, Sinae Kim, Isaac Yi Kim, Sharad Goyal","doi":"10.1097/IJ9.0000000000000013","DOIUrl":null,"url":null,"abstract":"<p><p>Little data exist on effect of undergoing laparoscopic prostatectomy(LP) versus open prostatectomy(OP) upon 30-day mortality rates among low-risk prostate cancer patients.</p><p><strong>Materials and methods: </strong>Using the National Cancer Database, we identified men (2004 to 2013) with biopsy-proven, low-risk prostate cancer who met the eligibility criteria: N0, M0, T-stage≤2A, PSA≤10 ng/mL, and Gleason score=6. We utilized a 1:N matched case-control study, with cases and controls matched by race, insurance status, Charlson-Deyo comorbidity score, surgical margin status, and facility type to investigate the short-term comparative effectiveness of LP versus OP.</p><p><strong>Results: </strong>Among the 448,773 patients in the National Cancer Database with low-risk prostate cancer, 116,359 patients met the above inclusion criteria. The target group was restricted to patients who received LP or OP, thus, leaving 44,720 patients for the study. The use of LP (compared with OP) was associated with patients with privately insured patients, treatment at an academic/research centers, high-volume hospitals, and white race (all <i>P</i><0.01). LP was less frequently utilized for black patients, those who received treatment at community centers, and for those with Medicaid insurance(all <i>P</i><0.01). The odds ratio of death for surgery type (laparoscopy vs. open) was estimated at 0.31 (95% confidence interval, 0.135-0.701; <i>P</i><0.05). Thus, the risk of death within 30 days was 69% lower with LP compared with OP.</p><p><strong>Conclusions: </strong>We found that the 30-day mortality rate among low-risk prostate cancer patients is significantly lower among patients who received LP when compared with OP, with various clinicopathologic parameters associated with its preferential use.</p>","PeriodicalId":42930,"journal":{"name":"International Journal of Surgery-Oncology","volume":"2 7","pages":"e13"},"PeriodicalIF":0.1000,"publicationDate":"2017-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1097/IJ9.0000000000000013","citationCount":"4","resultStr":"{\"title\":\"Comparative effectiveness of laparoscopic versus open prostatectomy for men with low-risk prostate cancer: a matched case-control study.\",\"authors\":\"Rahul R Parikh, Amil Patel, Sinae Kim, Isaac Yi Kim, Sharad Goyal\",\"doi\":\"10.1097/IJ9.0000000000000013\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Little data exist on effect of undergoing laparoscopic prostatectomy(LP) versus open prostatectomy(OP) upon 30-day mortality rates among low-risk prostate cancer patients.</p><p><strong>Materials and methods: </strong>Using the National Cancer Database, we identified men (2004 to 2013) with biopsy-proven, low-risk prostate cancer who met the eligibility criteria: N0, M0, T-stage≤2A, PSA≤10 ng/mL, and Gleason score=6. We utilized a 1:N matched case-control study, with cases and controls matched by race, insurance status, Charlson-Deyo comorbidity score, surgical margin status, and facility type to investigate the short-term comparative effectiveness of LP versus OP.</p><p><strong>Results: </strong>Among the 448,773 patients in the National Cancer Database with low-risk prostate cancer, 116,359 patients met the above inclusion criteria. The target group was restricted to patients who received LP or OP, thus, leaving 44,720 patients for the study. The use of LP (compared with OP) was associated with patients with privately insured patients, treatment at an academic/research centers, high-volume hospitals, and white race (all <i>P</i><0.01). LP was less frequently utilized for black patients, those who received treatment at community centers, and for those with Medicaid insurance(all <i>P</i><0.01). The odds ratio of death for surgery type (laparoscopy vs. open) was estimated at 0.31 (95% confidence interval, 0.135-0.701; <i>P</i><0.05). Thus, the risk of death within 30 days was 69% lower with LP compared with OP.</p><p><strong>Conclusions: </strong>We found that the 30-day mortality rate among low-risk prostate cancer patients is significantly lower among patients who received LP when compared with OP, with various clinicopathologic parameters associated with its preferential use.</p>\",\"PeriodicalId\":42930,\"journal\":{\"name\":\"International Journal of Surgery-Oncology\",\"volume\":\"2 7\",\"pages\":\"e13\"},\"PeriodicalIF\":0.1000,\"publicationDate\":\"2017-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1097/IJ9.0000000000000013\",\"citationCount\":\"4\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Journal of Surgery-Oncology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/IJ9.0000000000000013\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2017/7/5 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Surgery-Oncology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/IJ9.0000000000000013","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2017/7/5 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"ONCOLOGY","Score":null,"Total":0}
Comparative effectiveness of laparoscopic versus open prostatectomy for men with low-risk prostate cancer: a matched case-control study.
Little data exist on effect of undergoing laparoscopic prostatectomy(LP) versus open prostatectomy(OP) upon 30-day mortality rates among low-risk prostate cancer patients.
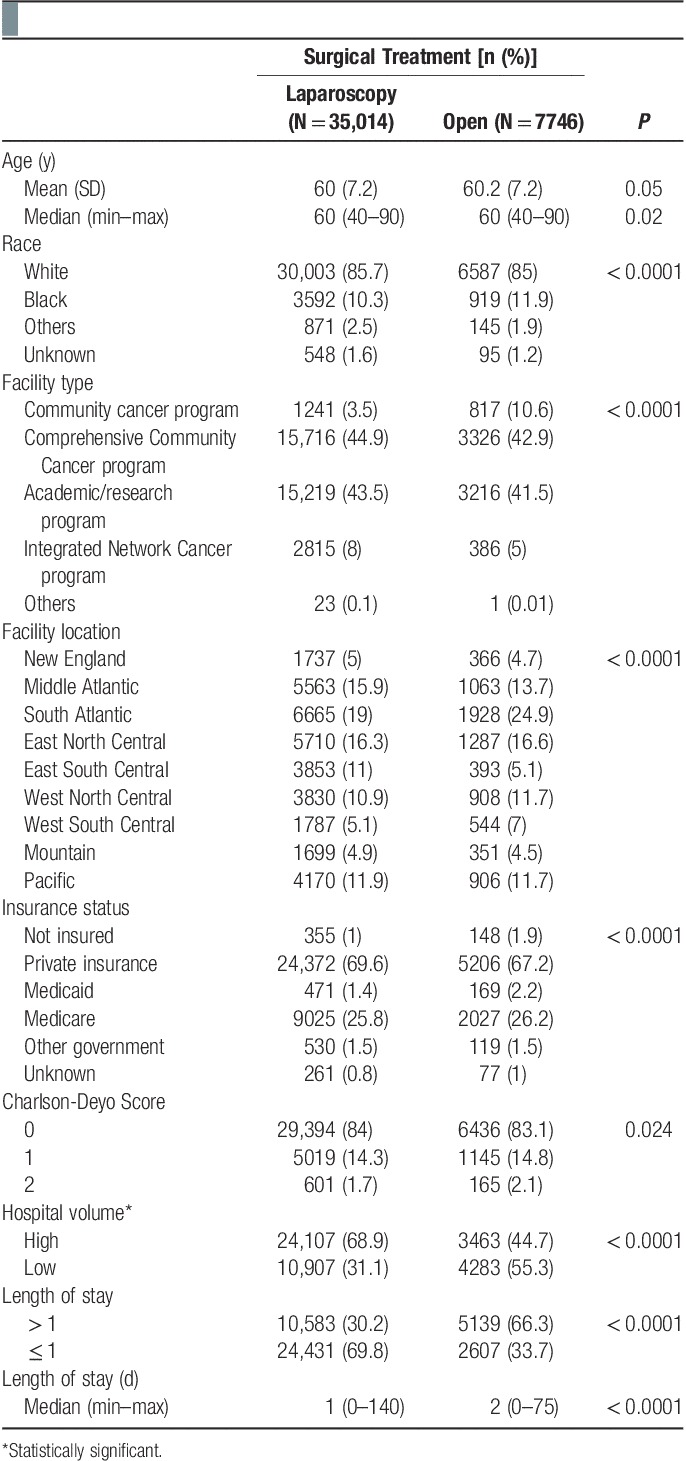
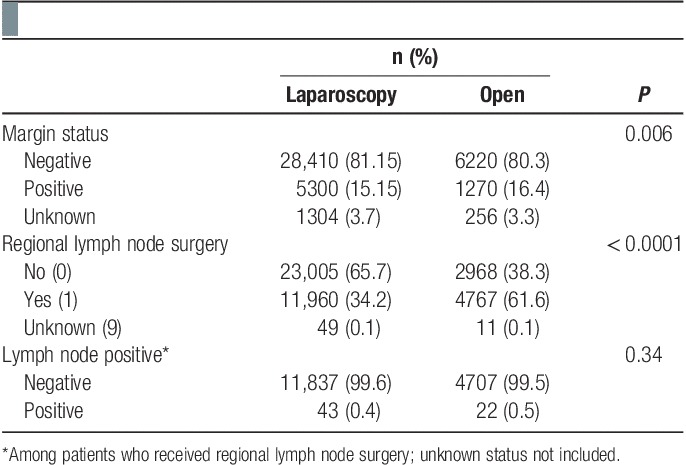
Materials and methods: Using the National Cancer Database, we identified men (2004 to 2013) with biopsy-proven, low-risk prostate cancer who met the eligibility criteria: N0, M0, T-stage≤2A, PSA≤10 ng/mL, and Gleason score=6. We utilized a 1:N matched case-control study, with cases and controls matched by race, insurance status, Charlson-Deyo comorbidity score, surgical margin status, and facility type to investigate the short-term comparative effectiveness of LP versus OP.
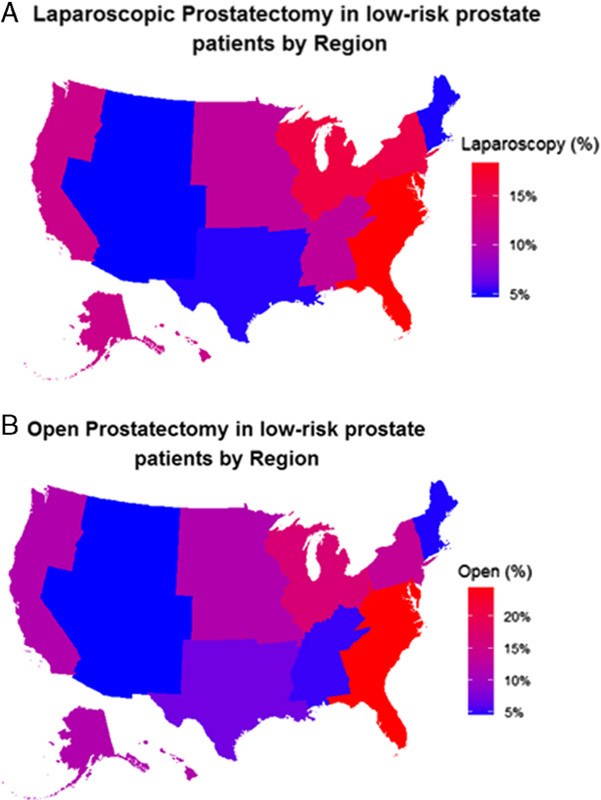
Results: Among the 448,773 patients in the National Cancer Database with low-risk prostate cancer, 116,359 patients met the above inclusion criteria. The target group was restricted to patients who received LP or OP, thus, leaving 44,720 patients for the study. The use of LP (compared with OP) was associated with patients with privately insured patients, treatment at an academic/research centers, high-volume hospitals, and white race (all P<0.01). LP was less frequently utilized for black patients, those who received treatment at community centers, and for those with Medicaid insurance(all P<0.01). The odds ratio of death for surgery type (laparoscopy vs. open) was estimated at 0.31 (95% confidence interval, 0.135-0.701; P<0.05). Thus, the risk of death within 30 days was 69% lower with LP compared with OP.
Conclusions: We found that the 30-day mortality rate among low-risk prostate cancer patients is significantly lower among patients who received LP when compared with OP, with various clinicopathologic parameters associated with its preferential use.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


