{"title":"使用GORE CARDIOFORM房间隔封堵器(GCSO)经导管房间隔缺损闭合1例婴儿(体重6.4 kg)。","authors":"Roman Scheidmann, Thomas Paul, Matthias Sigler","doi":"10.1186/s40348-017-0077-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Transcatheter closure has become the treatment of choice for secundum atrial septal defects (ASD II), but particularly in small children, there is concern regarding procedure-related complications.</p><p><strong>Case description: </strong>We report on a 10-month-old infant, body weight of 6.4 kg, with a large ASD who was referred for failure to thrive and dyspnea on exertion. Echocardiography showed two neighboring ASDs centrally located within an atrial septum with a length of 27 mm resulting in significant left-to-right shunting. During cardiac catheterization, hemodynamic significance of the defect as well as normal pulmonary vascular resistance was demonstrated. Balloon sizing of the central ASD showed a stretched defect diameter of 12 × 11 mm. A 20-mm GORE CARDIOFORM septal occluder (GCSO; Goremedical, W. L. Gore & Associates, Inc., Newark, DE, USA) was implanted without any complications. Initial trivial residual shunting resolved during 4 months of follow-up. Right ventricular dimensions declined significantly, and the boy gained body weight properly.</p><p><strong>Discussion, evaluation and conclusion: </strong>As demonstrated in our report, even large ASDs can be closed safely by catheter intervention in small infants. Selection of implant device and optimal sizing is of paramount importance. The size of the delivery sheath (11 French in our patient) is a potential limitation for the GCSO in smaller infants.</p>","PeriodicalId":74215,"journal":{"name":"Molecular and cellular pediatrics","volume":"4 1","pages":"9"},"PeriodicalIF":2.4000,"publicationDate":"2017-11-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/s40348-017-0077-7","citationCount":"4","resultStr":"{\"title\":\"Transcatheter atrial septal defect closure in an infant (body weight 6.4 kg) using the GORE CARDIOFORM septal occluder (GCSO).\",\"authors\":\"Roman Scheidmann, Thomas Paul, Matthias Sigler\",\"doi\":\"10.1186/s40348-017-0077-7\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Transcatheter closure has become the treatment of choice for secundum atrial septal defects (ASD II), but particularly in small children, there is concern regarding procedure-related complications.</p><p><strong>Case description: </strong>We report on a 10-month-old infant, body weight of 6.4 kg, with a large ASD who was referred for failure to thrive and dyspnea on exertion. Echocardiography showed two neighboring ASDs centrally located within an atrial septum with a length of 27 mm resulting in significant left-to-right shunting. During cardiac catheterization, hemodynamic significance of the defect as well as normal pulmonary vascular resistance was demonstrated. Balloon sizing of the central ASD showed a stretched defect diameter of 12 × 11 mm. A 20-mm GORE CARDIOFORM septal occluder (GCSO; Goremedical, W. L. Gore & Associates, Inc., Newark, DE, USA) was implanted without any complications. Initial trivial residual shunting resolved during 4 months of follow-up. Right ventricular dimensions declined significantly, and the boy gained body weight properly.</p><p><strong>Discussion, evaluation and conclusion: </strong>As demonstrated in our report, even large ASDs can be closed safely by catheter intervention in small infants. Selection of implant device and optimal sizing is of paramount importance. The size of the delivery sheath (11 French in our patient) is a potential limitation for the GCSO in smaller infants.</p>\",\"PeriodicalId\":74215,\"journal\":{\"name\":\"Molecular and cellular pediatrics\",\"volume\":\"4 1\",\"pages\":\"9\"},\"PeriodicalIF\":2.4000,\"publicationDate\":\"2017-11-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1186/s40348-017-0077-7\",\"citationCount\":\"4\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Molecular and cellular pediatrics\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s40348-017-0077-7\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"PEDIATRICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Molecular and cellular pediatrics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40348-017-0077-7","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 4
摘要
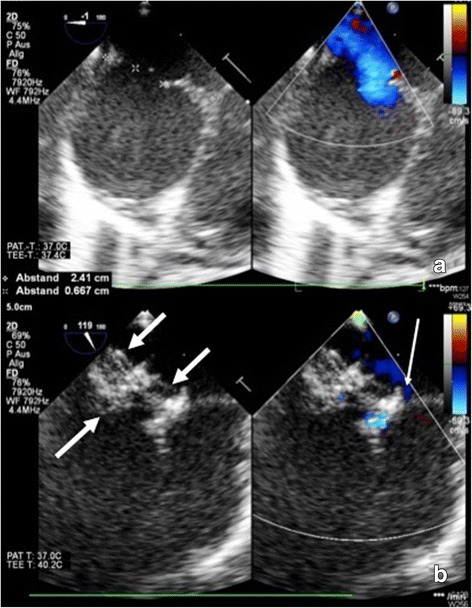
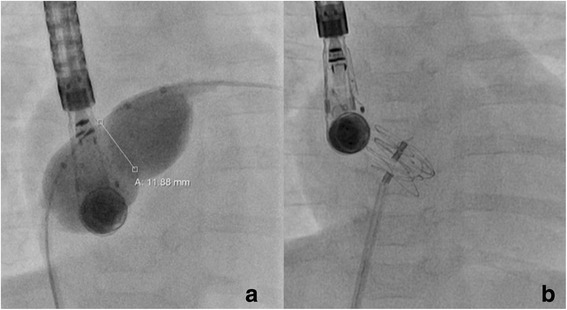
导论:经导管闭合术已成为治疗继发性房间隔缺损(ASD II)的首选方法,但特别是在幼儿中,存在手术相关并发症的担忧。病例描述:我们报告了一个10个月大的婴儿,体重6.4 kg,患有严重的ASD,因发育不全和用力呼吸困难而被转诊。超声心动图显示两个相邻的asd位于房间隔中心,长度为27mm,导致明显的左向右分流。在心导管术中,证实了缺损的血流动力学意义以及正常的肺血管阻力。中心ASD的球囊大小显示拉伸缺陷直径为12 × 11 mm。20mm GORE心型间隔闭塞器(GCSO;Goremedical, W. L. Gore & Associates, Inc. Newark, DE, USA)植入无任何并发症。最初轻微的残余分流在4个月的随访中得到解决。右心室尺寸明显减小,男孩体重正常增加。讨论、评价和结论:在我们的报告中,即使是大的asd也可以通过导管介入在小婴儿中安全地闭合。选择植入装置和最佳尺寸是至关重要的。分娩鞘的大小(在本例患者中为11 French)是小婴儿GCSO的潜在限制因素。
Transcatheter atrial septal defect closure in an infant (body weight 6.4 kg) using the GORE CARDIOFORM septal occluder (GCSO).
Introduction: Transcatheter closure has become the treatment of choice for secundum atrial septal defects (ASD II), but particularly in small children, there is concern regarding procedure-related complications.
Case description: We report on a 10-month-old infant, body weight of 6.4 kg, with a large ASD who was referred for failure to thrive and dyspnea on exertion. Echocardiography showed two neighboring ASDs centrally located within an atrial septum with a length of 27 mm resulting in significant left-to-right shunting. During cardiac catheterization, hemodynamic significance of the defect as well as normal pulmonary vascular resistance was demonstrated. Balloon sizing of the central ASD showed a stretched defect diameter of 12 × 11 mm. A 20-mm GORE CARDIOFORM septal occluder (GCSO; Goremedical, W. L. Gore & Associates, Inc., Newark, DE, USA) was implanted without any complications. Initial trivial residual shunting resolved during 4 months of follow-up. Right ventricular dimensions declined significantly, and the boy gained body weight properly.
Discussion, evaluation and conclusion: As demonstrated in our report, even large ASDs can be closed safely by catheter intervention in small infants. Selection of implant device and optimal sizing is of paramount importance. The size of the delivery sheath (11 French in our patient) is a potential limitation for the GCSO in smaller infants.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


