Paula S Lee, Samantha Kempner, Michael Miller, Jennifer Dominguez, Chad Grotegut, Jessie Ehrisman, Rebecca Previs, Laura J Havrilesky, Gloria Broadwater, Sarah C Ellestad, Angeles Alvarez Secord
{"title":"采用多学科方法处理产前疑似胎盘:最新算法和患者预后。","authors":"Paula S Lee, Samantha Kempner, Michael Miller, Jennifer Dominguez, Chad Grotegut, Jessie Ehrisman, Rebecca Previs, Laura J Havrilesky, Gloria Broadwater, Sarah C Ellestad, Angeles Alvarez Secord","doi":"10.1186/s40661-017-0049-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Due to the significant morbidity and mortality associated with placenta percreta, alternative management options are needed. Beginning in 2005, our institution implemented a multidisciplinary strategy to patients with suspected placenta percreta. The purpose of this study is to present our current strategy, maternal morbidity and outcomes of patients treated by our approach.</p><p><strong>Methods: </strong>From 2005 to 2014, a retrospective cohort study of patients with suspected placenta percreta at an academic tertiary care institution was performed. Treatment modalities included immediate hysterectomy at the time of cesarean section (CHYS), planned delayed hysterectomy (interval hysterectomy 6 weeks after delivery) (DH), and fertility sparing (uterine conservation) (FS). Prognostic factors of maternal morbidity were identified from medical records. Complications directly related to interventional procedures and DH was recorded. Descriptive statistics were utilized.</p><p><strong>Results: </strong>Of the 21 patients with suspected placenta percreta, 7 underwent CHYS, 13 underwent DH, and 1 had FS with uterine preservation. Of the 20 cases that underwent hysterectomy, final pathology showed 11 increta, 7 percreta, and 2 inconclusive. 19/20 cases underwent interventional radiology (IR) procedures. Selective embolization was utilized in 14 cases (2/7 CHYS; 12/13 DH). The median time from cesarean section (CS) to DH was 41 [26-68] days. There were no cases of emergent hysterectomy, delayed hemorrhage, or sepsis in the DH group. Both estimated blood loss and number of packed red blood cell transfusions were significantly higher in the CHYS group. 3/21 cases required massive transfusion (2 CHYS, 1 FS) with median total blood product transfusion of 13 units [12-15]. The four IR-related complications occurred in the DH group. Incidence of postoperative complications was similar between both groups. Median hospital length of stay (LOS) after CHYS was 4 days [3-8] compared to DH cohort: 7 days [3-33] after CS and 4 days [1 -10] after DH. The DH cohort had a higher rate of hospital readmission of 54% (7/13) compared to 14% (1/7) CHYS, most commonly due to pain. There were no maternal deaths.</p><p><strong>Conclusion: </strong>This multidisciplinary strategy may appear feasible; however, further investigation is warranted to evaluate the effectiveness of alternative approaches to cesarean hysterectomy in cases of morbidly adherent placenta.</p>","PeriodicalId":91487,"journal":{"name":"Gynecologic oncology research and practice","volume":"4 ","pages":"11"},"PeriodicalIF":0.0000,"publicationDate":"2017-08-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5567476/pdf/","citationCount":"0","resultStr":"{\"title\":\"Multidisciplinary approach to manage antenatally suspected placenta percreta: updated algorithm and patient outcomes.\",\"authors\":\"Paula S Lee, Samantha Kempner, Michael Miller, Jennifer Dominguez, Chad Grotegut, Jessie Ehrisman, Rebecca Previs, Laura J Havrilesky, Gloria Broadwater, Sarah C Ellestad, Angeles Alvarez Secord\",\"doi\":\"10.1186/s40661-017-0049-6\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Due to the significant morbidity and mortality associated with placenta percreta, alternative management options are needed. Beginning in 2005, our institution implemented a multidisciplinary strategy to patients with suspected placenta percreta. The purpose of this study is to present our current strategy, maternal morbidity and outcomes of patients treated by our approach.</p><p><strong>Methods: </strong>From 2005 to 2014, a retrospective cohort study of patients with suspected placenta percreta at an academic tertiary care institution was performed. Treatment modalities included immediate hysterectomy at the time of cesarean section (CHYS), planned delayed hysterectomy (interval hysterectomy 6 weeks after delivery) (DH), and fertility sparing (uterine conservation) (FS). Prognostic factors of maternal morbidity were identified from medical records. Complications directly related to interventional procedures and DH was recorded. Descriptive statistics were utilized.</p><p><strong>Results: </strong>Of the 21 patients with suspected placenta percreta, 7 underwent CHYS, 13 underwent DH, and 1 had FS with uterine preservation. Of the 20 cases that underwent hysterectomy, final pathology showed 11 increta, 7 percreta, and 2 inconclusive. 19/20 cases underwent interventional radiology (IR) procedures. Selective embolization was utilized in 14 cases (2/7 CHYS; 12/13 DH). The median time from cesarean section (CS) to DH was 41 [26-68] days. There were no cases of emergent hysterectomy, delayed hemorrhage, or sepsis in the DH group. Both estimated blood loss and number of packed red blood cell transfusions were significantly higher in the CHYS group. 3/21 cases required massive transfusion (2 CHYS, 1 FS) with median total blood product transfusion of 13 units [12-15]. The four IR-related complications occurred in the DH group. Incidence of postoperative complications was similar between both groups. Median hospital length of stay (LOS) after CHYS was 4 days [3-8] compared to DH cohort: 7 days [3-33] after CS and 4 days [1 -10] after DH. The DH cohort had a higher rate of hospital readmission of 54% (7/13) compared to 14% (1/7) CHYS, most commonly due to pain. There were no maternal deaths.</p><p><strong>Conclusion: </strong>This multidisciplinary strategy may appear feasible; however, further investigation is warranted to evaluate the effectiveness of alternative approaches to cesarean hysterectomy in cases of morbidly adherent placenta.</p>\",\"PeriodicalId\":91487,\"journal\":{\"name\":\"Gynecologic oncology research and practice\",\"volume\":\"4 \",\"pages\":\"11\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2017-08-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5567476/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Gynecologic oncology research and practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s40661-017-0049-6\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2017/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Gynecologic oncology research and practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40661-017-0049-6","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2017/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Multidisciplinary approach to manage antenatally suspected placenta percreta: updated algorithm and patient outcomes.
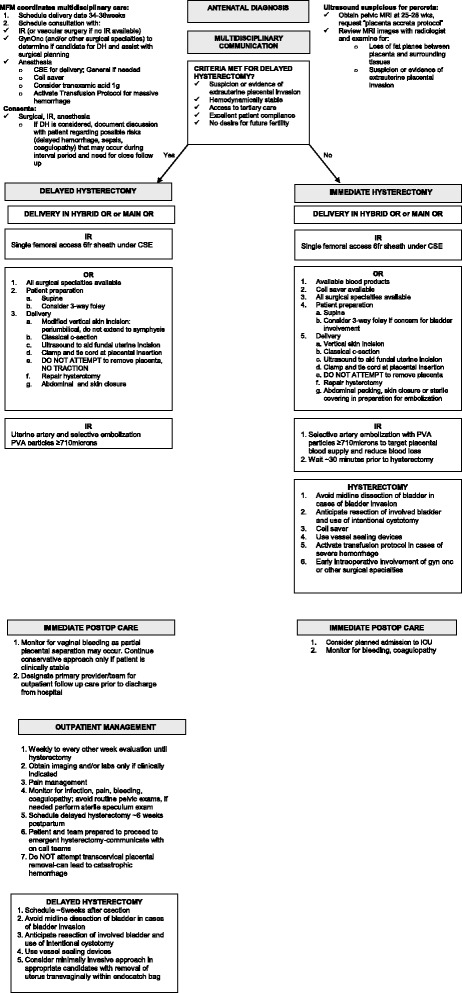
Background: Due to the significant morbidity and mortality associated with placenta percreta, alternative management options are needed. Beginning in 2005, our institution implemented a multidisciplinary strategy to patients with suspected placenta percreta. The purpose of this study is to present our current strategy, maternal morbidity and outcomes of patients treated by our approach.
Methods: From 2005 to 2014, a retrospective cohort study of patients with suspected placenta percreta at an academic tertiary care institution was performed. Treatment modalities included immediate hysterectomy at the time of cesarean section (CHYS), planned delayed hysterectomy (interval hysterectomy 6 weeks after delivery) (DH), and fertility sparing (uterine conservation) (FS). Prognostic factors of maternal morbidity were identified from medical records. Complications directly related to interventional procedures and DH was recorded. Descriptive statistics were utilized.
Results: Of the 21 patients with suspected placenta percreta, 7 underwent CHYS, 13 underwent DH, and 1 had FS with uterine preservation. Of the 20 cases that underwent hysterectomy, final pathology showed 11 increta, 7 percreta, and 2 inconclusive. 19/20 cases underwent interventional radiology (IR) procedures. Selective embolization was utilized in 14 cases (2/7 CHYS; 12/13 DH). The median time from cesarean section (CS) to DH was 41 [26-68] days. There were no cases of emergent hysterectomy, delayed hemorrhage, or sepsis in the DH group. Both estimated blood loss and number of packed red blood cell transfusions were significantly higher in the CHYS group. 3/21 cases required massive transfusion (2 CHYS, 1 FS) with median total blood product transfusion of 13 units [12-15]. The four IR-related complications occurred in the DH group. Incidence of postoperative complications was similar between both groups. Median hospital length of stay (LOS) after CHYS was 4 days [3-8] compared to DH cohort: 7 days [3-33] after CS and 4 days [1 -10] after DH. The DH cohort had a higher rate of hospital readmission of 54% (7/13) compared to 14% (1/7) CHYS, most commonly due to pain. There were no maternal deaths.
Conclusion: This multidisciplinary strategy may appear feasible; however, further investigation is warranted to evaluate the effectiveness of alternative approaches to cesarean hysterectomy in cases of morbidly adherent placenta.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


