滤泡性淋巴瘤转化为高级别b细胞淋巴瘤,伴有MYC和BCL2易位以及Burkitt淋巴瘤和急性淋巴细胞白血病的重叠特征:1例报告和文献复习
摘要
最常见的是,滤泡性淋巴瘤(FL)的组织学转化(HT)表现为弥漫性大b细胞淋巴瘤,没有其他特异性(DLBCL, NOS)。不太常见的是,HT可能导致MYC和b细胞淋巴瘤蛋白2 (BCL2)和/或BCL6基因重排的高级别b细胞淋巴瘤(HGBL),也被称为“双击”或“三击”淋巴瘤。在2016年修订的世界卫生组织(WHO)淋巴样肿瘤分类中,由于标准模糊和诊断效益有限,b细胞淋巴瘤这一不可分类的类别被取消。相反,世卫组织引入了HGBL类别,其特征是MYC和BCL2和/或BCL6重排。表现为DLBCL和伯基特淋巴瘤(BL)中间表型的病例将属于HGBL类别。在非常罕见的情况下,HT同时导致中度大细胞淋巴瘤和BL表型,并表现出淋巴母细胞特征,在这种情况下,世卫组织建议应注意这种形态学表现。与新发DLBCL、NOS患者相比,MYC、BCL2和/或BCL6基因重排患者预后更差。一名63岁女性,表现为左颈部腺病。实验室评估包括全血细胞计数、全代谢组、血清乳酸脱氢酶和β2微球蛋白均正常。全身计算机断层扫描(CT)显示横膈膜上下弥漫性腺病变。切除淋巴结活检显示3A级结节性FL。Ki67标记指数为40% ~ 50%。骨髓活组织检查显示小结节旁CD20+淋巴样聚集体。患者接受6个周期苯达莫司汀(+1和+2天90mg /m2)和利妥昔单抗(+2天375 mg/m2),每4周给药一次。治疗结束后的随访CT扫描显示腋窝腺病的消退和腹膜后大淋巴结的显著缩小。18个月后,她在没有B症状的情况下出现腹痛。正电子发射断层扫描与2-脱氧-2-[氟-18]氟-d-葡萄糖结合CT (18F-FDG PET/CT)扫描显示广泛的腺病变,弥漫性脾受累和大量骨髓受累。2.4 cm右腋窝淋巴结活检(SUVmax为16.1)显示3A级FL累及,以结节型生长为主。骨髓活检再次显示只有小病灶FL。她于2015年5月开始接受理想拉昔布(150mg,每日两次)和利妥昔单抗(375 mg/m2,每月)治疗。4个周期后,重复CT扫描显示完全的x线片反应。随后,Idelalisib因免疫介导性结肠炎接受皮质类固醇治疗。一个月后,她重新开始使用ideelalisib,剂量减少了50%。2周后,她回到诊所,主诉双侧髋关节和下腰椎不适,但没有B症状。2016年1月复查18F-FDG PET/CT显示骨髓摄取显著。骨髓穿刺显示肿瘤细胞片,从具有淋巴母细胞特征的中等大小的细胞到具有多个核仁的非常大的非典型细胞。存在两种不同的组织学;一个与患者已知的以结节为主的FL一致,另一个与HT一致(大的非典型细胞表达PAX5、CD10、BCL2和c-MYC, CD20、MPO、CD34、CD30和BCL6阴性)。病灶区域在凝块切片上可见微弱的、不均匀的末端脱氧核苷酸转移酶表达。Ki67增殖指数高(4+/4)。荧光原位杂交分析显示,2个群体存在MYC扩增和/或重排,未发现BCL6重排;核型分析显示一个复杂的异常女性核型与t(14;18)和多个结构和数字异常。她开始服用剂量调整的利妥昔单抗、依托泊苷、强的松、长春新碱、环磷酰胺和阿霉素,同时预防性鞘内注射甲氨蝶呤和阿糖胞苷。在她死于进行性淋巴瘤之前,她只有短暂的反应。ideelalisib是否能为选择更具攻击性的克隆提供一个微环境需要解决。本例患者的临床过程因ideelalisib的掺入而混乱,同时因HT的复杂性和一线化疗方案影响双重打击淋巴瘤的机制而进一步复杂化。
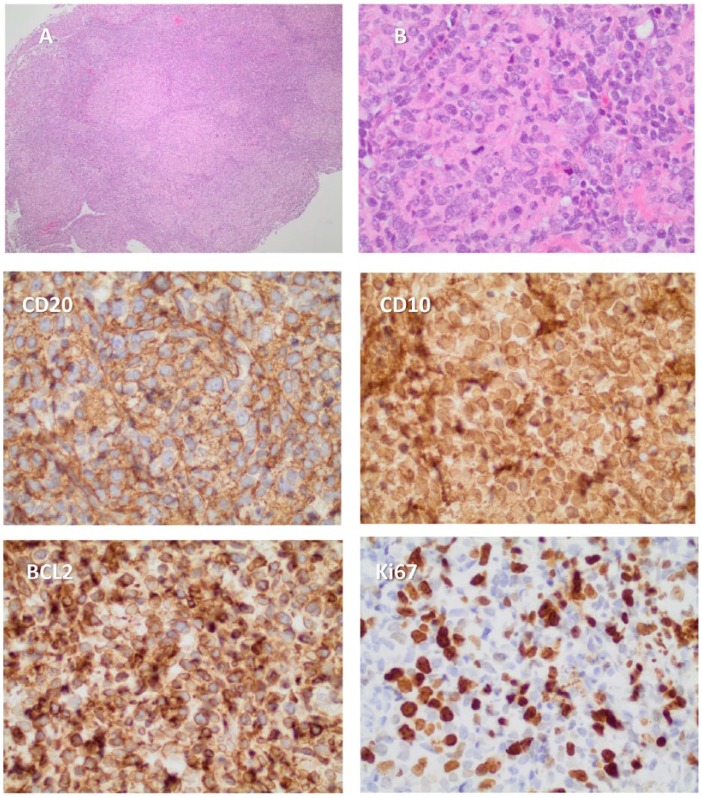
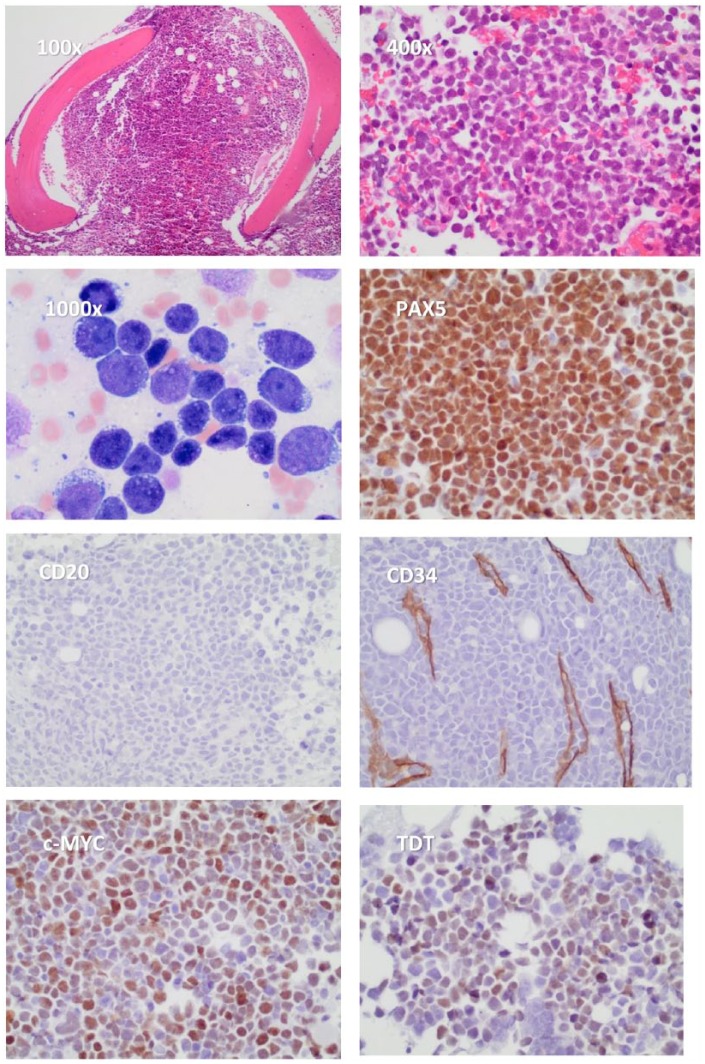
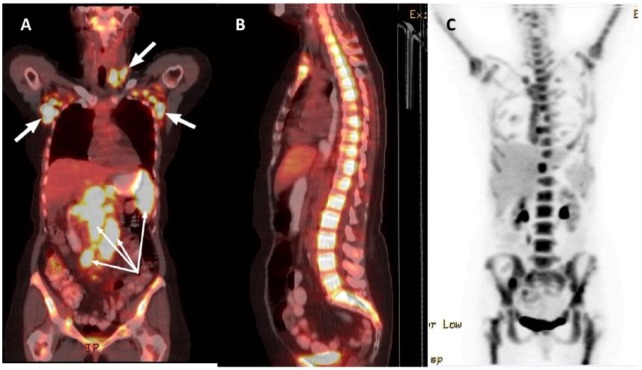
Most commonly, histologic transformation (HT) from follicular lymphoma (FL) manifests as a diffuse large B-cell lymphoma, not otherwise specified (DLBCL, NOS). Less frequently, HT may result in a high-grade B-cell lymphoma (HGBL) with MYC and B-cell lymphoma protein 2 (BCL2) and/or BCL6 gene rearrangements, also known as "double-hit" or "triple-hit" lymphomas. In the 2016 revision of the World Health Organization (WHO) classification of lymphoid neoplasms, the category B-cell lymphoma, unclassifiable was eliminated due to its vague criteria and limiting diagnostic benefit. Instead, the WHO introduced the HGBL category, characterized by MYC and BCL2 and/or BCL6 rearrangements. Cases that present as an intermediate phenotype of DLBCL and Burkitt lymphoma (BL) will fall within this HGBL category. Very rarely, HT results in both the intermediate DLBCL and BL phenotypes and exhibits lymphoblastic features, in which case the WHO recommends that this morphologic appearance should be noted. In comparison with de novo patients with DLBCL, NOS, those with MYC and BCL2 and/or BCL6 gene rearrangements have a worse prognosis. A 63-year-old woman presented with left neck adenopathy. Laboratory assessments, including complete blood count, complete metabolic panel, serum lactate dehydrogenase, and β2-microglobulin, were all normal. A whole-body computerized tomographic (CT) scan revealed diffuse adenopathy above and below the diaphragm. An excisional node biopsy showed grade 3A nodular FL. The Ki67 labeling index was 40% to 50%. A bone marrow biopsy showed a small focus of paratrabecular CD20+ lymphoid aggregates. She received 6 cycles of bendamustine (90 mg/m2 on days +1 and +2) and rituximab (375 mg/m2 on day +2), with each cycle delivered every 4 weeks. A follow-up CT scan at completion of therapy showed a partial response with resolution of axillary adenopathy and a dramatic shrinkage of the large retroperitoneal nodes. After 18 months, she had crampy abdominal pain in the absence of B symptoms. Positron emission tomography with 2-deoxy-2-[fluorine-18] fluoro-d-glucose integrated with CT (18F-FDG PET/CT) scan showed widespread adenopathy, diffuse splenic involvement, and substantial marrow involvement. Biopsy of a 2.4-cm right axillary node (SUVmax of 16.1) showed involvement by grade 3A FL with a predominant nodular pattern of growth. A bone marrow biopsy once again showed only a small focus of FL. She received idelalisib (150 mg twice daily) and rituximab (375 mg/m2, monthly) beginning May 2015. After 4 cycles, a repeat CT scan showed a complete radiographic response. Idelalisib was subsequently held while she received corticosteroids for immune-mediated colitis. A month later, she restarted idelalisib with a 50% dose reduction. After 2 weeks, she returned to clinic complaining of bilateral hip and low lumbar discomfort but no B symptoms. A restaging 18F-FDG PET/CT in January 2016 showed dramatic marrow uptake. A bone marrow aspirate showed sheets of tumor cells representing a spectrum from intermediate-sized cells with lymphoblastic features to very large atypical cells with multiple nucleoli. Two distinct histologies were present; one remained consistent with the patient's known FL with a predominant nodular pattern and the other consistent with HT (the large atypical cells expressed PAX5, CD10, BCL2, and c-MYC and were negative for CD20, MPO, CD34, CD30, and BCL6). Focal areas showed faint, heterogeneous expression of terminal deoxynucleotidyl transferase best seen on the clot section. Ki67 proliferation index was high (4+/4). Fluorescence in situ hybridization analysis showed 2 populations with MYC amplification and/or rearrangement and no evidence of BCL6 rearrangement; a karyotype analysis showed a complex abnormal female karyotype with t(14;18) and multiple structural and numerical abnormalities. She started dose-adjusted rituximab, etoposide, prednisone, vincristine, cyclophosphamide, and doxorubicin with concomitant prophylactic intrathecal methotrexate and cytarabine. She had but a short-lived response before dying in hospice from progressive lymphoma. Whether idelalisib could provide a microenvironment for selection of more aggressive clones needs to be addressed. Our patient's clinical course is confounded by the incorporation of idelalisib while being further complicated by the complexity of HT and the mechanisms in which first-line chemotherapy regimens affect double-hit lymphoma.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


