Mae Johnson, Martin Whyte, Robert Loveridge, Richard Yorke, Shairana Naleem
{"title":"用于心肺复苏术和紧急治疗升级计划的统一电子工具改善了急性住院患者的沟通和早期协作决策。","authors":"Mae Johnson, Martin Whyte, Robert Loveridge, Richard Yorke, Shairana Naleem","doi":"10.1136/bmjquality.u213254.w6626","DOIUrl":null,"url":null,"abstract":"<p><p>The National Confidential Enquiry into Patient Outcomes and Death (NCEPOD) report 'Time to Intervene' (2012) stated that in a substantial number of cases, resuscitation is attempted when it was thought a 'do not attempt cardiopulmonary resuscitation' (DNACPR) decision should have been in place. Early decisions about CPR status and advance planning about limits of care now form part of national recommendations by the UK Resuscitation Council (2016). Treatment escalation plans (TEP) document what level of treatment intervention would be appropriate if a patient were to become acutely unwell and were not previously formally in place at King's College Hospital. A unifying paper based form was successfully piloted in the Acute Medical Unit, introducing the TEP and bringing together decision making around both treatment escalation and CPR status. Subsequently an electronic order-set for CPR status and treatment escalation was launched in April 2015 which led to a highly visible CPR and escalation status banner on the main screen at the top of the patient's electronic record. Ultimately due to further iterations in the electronic process by December 2016, all escalation decisions for acutely admitted patients now have high quality supporting, explanatory documentation with 100% having TEPs in place. There is now widespread multidisciplinary engagement in the process of defining limits of care for acutely admitted medical patients within the first 14 hours of admission and a strategy for rolling this process out across all the divisions of the hospital through our Deteriorating Patient Group (DPG). The collaborative design with acute medical, palliative and intensive care teams and the high visibility provided by the electronic process in the Electronic Patient Record (EPR) has enhanced communication with these teams, patients, nursing staff and the multidisciplinary team by ensuring clarity through a universally understood process about escalation and CPR. Clarity and openness about these discussions have been welcomed by patient focus groups facilitated via our acute medicine patient experience committee. There has been a shift in medical culture where transparency about limits of care has contributed to improving patient safety and quality of care through reducing unnecessary CPR supported by focus groups of staff.</p>","PeriodicalId":91218,"journal":{"name":"BMJ quality improvement reports","volume":"6 1","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2017-04-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1136/bmjquality.u213254.w6626","citationCount":"9","resultStr":"{\"title\":\"A Unified Electronic Tool for CPR and Emergency Treatment Escalation Plans Improves Communication and Early Collaborative Decision Making for Acute Hospital Admissions.\",\"authors\":\"Mae Johnson, Martin Whyte, Robert Loveridge, Richard Yorke, Shairana Naleem\",\"doi\":\"10.1136/bmjquality.u213254.w6626\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>The National Confidential Enquiry into Patient Outcomes and Death (NCEPOD) report 'Time to Intervene' (2012) stated that in a substantial number of cases, resuscitation is attempted when it was thought a 'do not attempt cardiopulmonary resuscitation' (DNACPR) decision should have been in place. Early decisions about CPR status and advance planning about limits of care now form part of national recommendations by the UK Resuscitation Council (2016). Treatment escalation plans (TEP) document what level of treatment intervention would be appropriate if a patient were to become acutely unwell and were not previously formally in place at King's College Hospital. A unifying paper based form was successfully piloted in the Acute Medical Unit, introducing the TEP and bringing together decision making around both treatment escalation and CPR status. Subsequently an electronic order-set for CPR status and treatment escalation was launched in April 2015 which led to a highly visible CPR and escalation status banner on the main screen at the top of the patient's electronic record. Ultimately due to further iterations in the electronic process by December 2016, all escalation decisions for acutely admitted patients now have high quality supporting, explanatory documentation with 100% having TEPs in place. There is now widespread multidisciplinary engagement in the process of defining limits of care for acutely admitted medical patients within the first 14 hours of admission and a strategy for rolling this process out across all the divisions of the hospital through our Deteriorating Patient Group (DPG). The collaborative design with acute medical, palliative and intensive care teams and the high visibility provided by the electronic process in the Electronic Patient Record (EPR) has enhanced communication with these teams, patients, nursing staff and the multidisciplinary team by ensuring clarity through a universally understood process about escalation and CPR. Clarity and openness about these discussions have been welcomed by patient focus groups facilitated via our acute medicine patient experience committee. There has been a shift in medical culture where transparency about limits of care has contributed to improving patient safety and quality of care through reducing unnecessary CPR supported by focus groups of staff.</p>\",\"PeriodicalId\":91218,\"journal\":{\"name\":\"BMJ quality improvement reports\",\"volume\":\"6 1\",\"pages\":\"\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2017-04-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1136/bmjquality.u213254.w6626\",\"citationCount\":\"9\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMJ quality improvement reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1136/bmjquality.u213254.w6626\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2017/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ quality improvement reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjquality.u213254.w6626","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2017/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
A Unified Electronic Tool for CPR and Emergency Treatment Escalation Plans Improves Communication and Early Collaborative Decision Making for Acute Hospital Admissions.
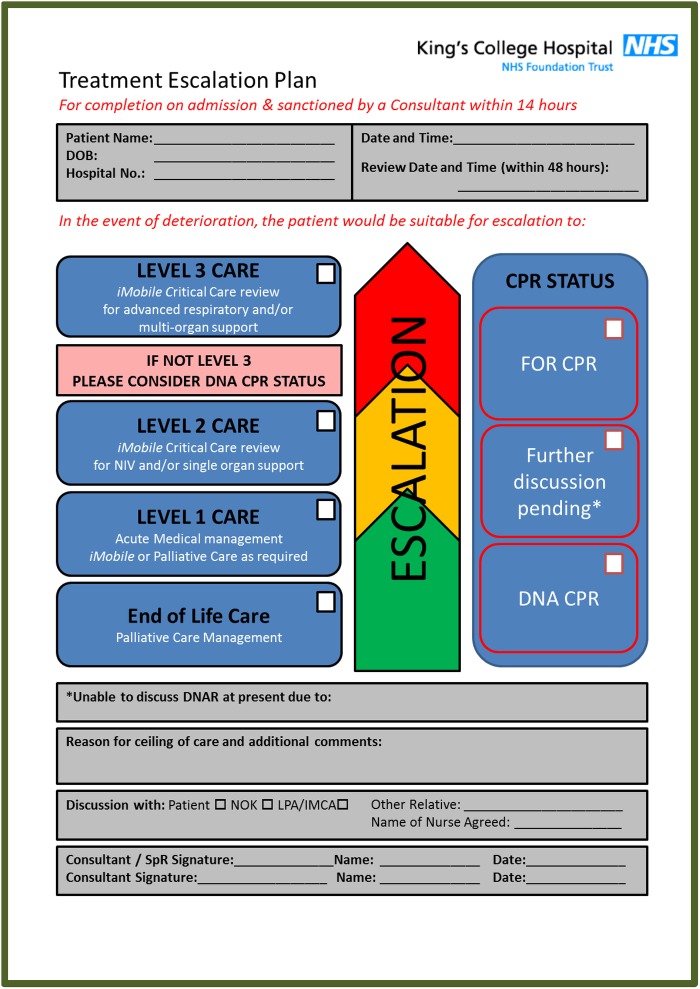
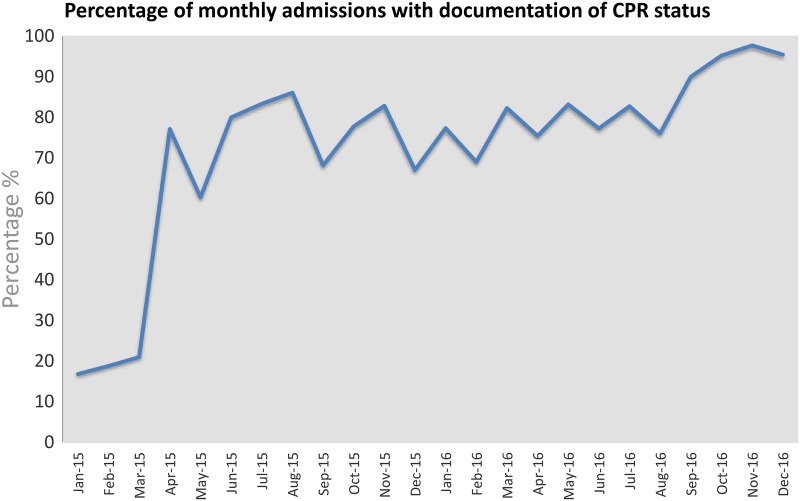
The National Confidential Enquiry into Patient Outcomes and Death (NCEPOD) report 'Time to Intervene' (2012) stated that in a substantial number of cases, resuscitation is attempted when it was thought a 'do not attempt cardiopulmonary resuscitation' (DNACPR) decision should have been in place. Early decisions about CPR status and advance planning about limits of care now form part of national recommendations by the UK Resuscitation Council (2016). Treatment escalation plans (TEP) document what level of treatment intervention would be appropriate if a patient were to become acutely unwell and were not previously formally in place at King's College Hospital. A unifying paper based form was successfully piloted in the Acute Medical Unit, introducing the TEP and bringing together decision making around both treatment escalation and CPR status. Subsequently an electronic order-set for CPR status and treatment escalation was launched in April 2015 which led to a highly visible CPR and escalation status banner on the main screen at the top of the patient's electronic record. Ultimately due to further iterations in the electronic process by December 2016, all escalation decisions for acutely admitted patients now have high quality supporting, explanatory documentation with 100% having TEPs in place. There is now widespread multidisciplinary engagement in the process of defining limits of care for acutely admitted medical patients within the first 14 hours of admission and a strategy for rolling this process out across all the divisions of the hospital through our Deteriorating Patient Group (DPG). The collaborative design with acute medical, palliative and intensive care teams and the high visibility provided by the electronic process in the Electronic Patient Record (EPR) has enhanced communication with these teams, patients, nursing staff and the multidisciplinary team by ensuring clarity through a universally understood process about escalation and CPR. Clarity and openness about these discussions have been welcomed by patient focus groups facilitated via our acute medicine patient experience committee. There has been a shift in medical culture where transparency about limits of care has contributed to improving patient safety and quality of care through reducing unnecessary CPR supported by focus groups of staff.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


