{"title":"减少股骨颈骨折患者的住院次数。","authors":"Selina Graham, Mark Dahill, Derek Robinson","doi":"10.1136/bmjquality.u215756.w6261","DOIUrl":null,"url":null,"abstract":"<p><p>The Royal United Hospital, Bath, admits approximately 550 patients with neck of femur fractures per year. The risks from returning to theatre for this patient group are often life-threatening. Post-operative wound ooze was noted to cause a significant rate of return to theatre, with increased lengths of stay and patient morbidity. A wound closure protocol was agreed by the consultant body. This information was disseminated by email and teaching sessions to all members of the multidisciplinary team, including surgeons, theatre staff and ortho-geriatricians. The plan-do-study-act model for improvement was used to reduce rates of returns to theatre for wound ooze. Interventions included cyclical teaching during each trainee rotation, updated inductions, posters, email reminders and scrub team involvement to open the protocol sutures unprompted. The primary outcome measure was returns to theatre for wound complications. Baseline data showed 4 returns to theatre over a two month period (4.40% of patients). Length of stay for each patient affected by wound ooze was also compared to the departmental mean. In the 6 month intervention period there was one return to theatre (0.36% of patients). The observed reduction saved the department an estimated £13,831 in length of stay alone. The standardisation of wound closure protocol, with continued reinforcement to all members of the multidisciplinary team, improves patient outcome in this group. Mobilising a group of clinicians across a variety of specialities, with one common goal, is highly effective for patients, improves multidisciplinary working and reduces cost.</p>","PeriodicalId":91218,"journal":{"name":"BMJ quality improvement reports","volume":"6 1","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2017-04-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1136/bmjquality.u215756.w6261","citationCount":"0","resultStr":"{\"title\":\"Reducing returns to theatre for neck of femur fracture patients.\",\"authors\":\"Selina Graham, Mark Dahill, Derek Robinson\",\"doi\":\"10.1136/bmjquality.u215756.w6261\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>The Royal United Hospital, Bath, admits approximately 550 patients with neck of femur fractures per year. The risks from returning to theatre for this patient group are often life-threatening. Post-operative wound ooze was noted to cause a significant rate of return to theatre, with increased lengths of stay and patient morbidity. A wound closure protocol was agreed by the consultant body. This information was disseminated by email and teaching sessions to all members of the multidisciplinary team, including surgeons, theatre staff and ortho-geriatricians. The plan-do-study-act model for improvement was used to reduce rates of returns to theatre for wound ooze. Interventions included cyclical teaching during each trainee rotation, updated inductions, posters, email reminders and scrub team involvement to open the protocol sutures unprompted. The primary outcome measure was returns to theatre for wound complications. Baseline data showed 4 returns to theatre over a two month period (4.40% of patients). Length of stay for each patient affected by wound ooze was also compared to the departmental mean. In the 6 month intervention period there was one return to theatre (0.36% of patients). The observed reduction saved the department an estimated £13,831 in length of stay alone. The standardisation of wound closure protocol, with continued reinforcement to all members of the multidisciplinary team, improves patient outcome in this group. Mobilising a group of clinicians across a variety of specialities, with one common goal, is highly effective for patients, improves multidisciplinary working and reduces cost.</p>\",\"PeriodicalId\":91218,\"journal\":{\"name\":\"BMJ quality improvement reports\",\"volume\":\"6 1\",\"pages\":\"\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2017-04-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1136/bmjquality.u215756.w6261\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMJ quality improvement reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1136/bmjquality.u215756.w6261\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2017/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ quality improvement reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjquality.u215756.w6261","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2017/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Reducing returns to theatre for neck of femur fracture patients.
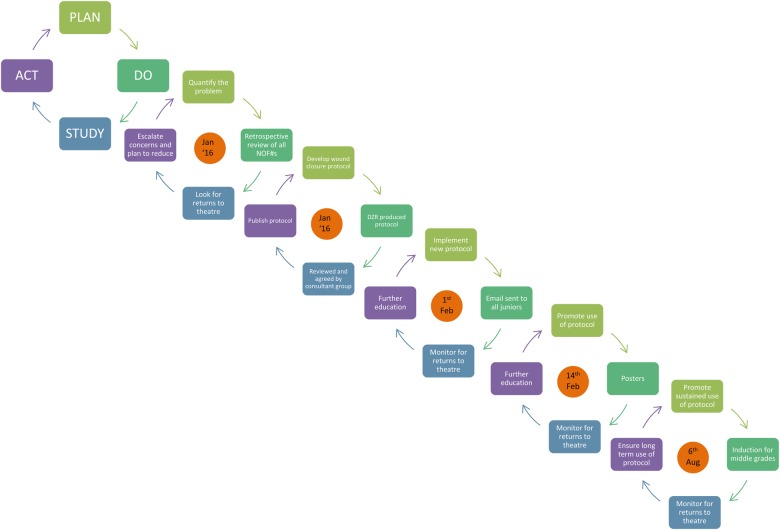
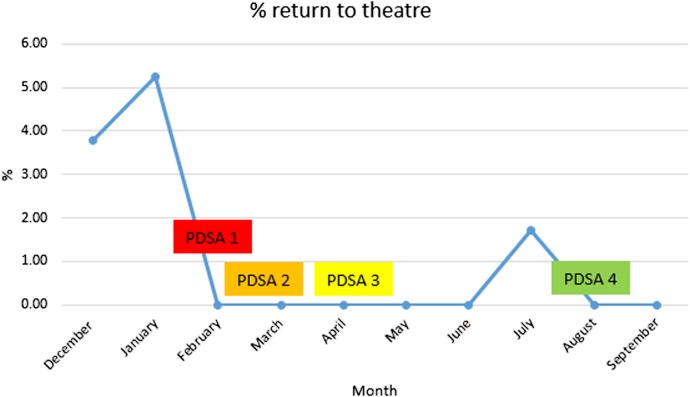
The Royal United Hospital, Bath, admits approximately 550 patients with neck of femur fractures per year. The risks from returning to theatre for this patient group are often life-threatening. Post-operative wound ooze was noted to cause a significant rate of return to theatre, with increased lengths of stay and patient morbidity. A wound closure protocol was agreed by the consultant body. This information was disseminated by email and teaching sessions to all members of the multidisciplinary team, including surgeons, theatre staff and ortho-geriatricians. The plan-do-study-act model for improvement was used to reduce rates of returns to theatre for wound ooze. Interventions included cyclical teaching during each trainee rotation, updated inductions, posters, email reminders and scrub team involvement to open the protocol sutures unprompted. The primary outcome measure was returns to theatre for wound complications. Baseline data showed 4 returns to theatre over a two month period (4.40% of patients). Length of stay for each patient affected by wound ooze was also compared to the departmental mean. In the 6 month intervention period there was one return to theatre (0.36% of patients). The observed reduction saved the department an estimated £13,831 in length of stay alone. The standardisation of wound closure protocol, with continued reinforcement to all members of the multidisciplinary team, improves patient outcome in this group. Mobilising a group of clinicians across a variety of specialities, with one common goal, is highly effective for patients, improves multidisciplinary working and reduces cost.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


