{"title":"使用电子医疗记录识别初级保健机构中的血脂异常患者:从一个地区到国家数据库的疾病代码事项的国际分类。","authors":"Justin Oake, Erfan Aref-Eshghi, Marshall Godwin, Kayla Collins, Kris Aubrey-Bassler, Pauline Duke, Masoud Mahdavian, Shabnam Asghari","doi":"10.1177/1178222616685880","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To assess the validity of the International Classification of Disease (ICD) codes for identifying patients with dyslipidemia in electronic medical record (EMR) data.</p><p><strong>Methods: </strong>The EMRs of patients receiving primary care in St. John's, Newfoundland and Labrador (NL), Canada, were retrieved from the Canadian Primary Care Sentinel Surveillance Network database. International Classification of Disease codes were first compared with laboratory lipid data as an independent criterion standard, and next with a \"comprehensive criterion standard,\" defined as any existence of abnormal lipid test, lipid-lowering medication record, or dyslipidemia ICD codes. The ability of ICD coding alone or combined with other components was evaluated against the two criterion standards using receiver operating characteristic (ROC) analysis, sensitivity, specificity, negative predictive value (NPV) and Kappa agreement. (No specificity was reported for the comparison of ICD codes against the comprehensive criterion standard as this naturally leads to 100% specificity.).</p><p><strong>Results: </strong>The ICD codes led to a poor outcome when compared with the serum lipid levels (sensitivity, 27%; specificity, 76%; PPV, 71%; NPV, 33%; Kappa, 0.02; area under the receiver operating characteristic curve (AUC), 0.51) or with the comprehensive criterion standard (sensitivity, 32%; NPV, 25%; Kappa, 0.15; AUC, 66%). International Classification of Disease codes combined with lipid-lowering medication data also resulted in low sensitivity (51.2%), NPV (32%), Kappa (0.28), and AUC (75%). The addition of laboratory lipid levels to ICD coding marginally improved the algorithm (sensitivity, 94%; NPV, 79%; Kappa, 0.85; AUC, 97%).</p><p><strong>Conclusions: </strong>The use of ICD coding, either alone or in combination with laboratory data or lipid-lowering medication records, was not an accurate indicator in identifying dyslipidemia.</p>","PeriodicalId":88397,"journal":{"name":"Biomedical informatics insights","volume":"9 ","pages":"1178222616685880"},"PeriodicalIF":0.0000,"publicationDate":"2017-02-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1177/1178222616685880","citationCount":"18","resultStr":"{\"title\":\"Using Electronic Medical Record to Identify Patients With Dyslipidemia in Primary Care Settings: International Classification of Disease Code Matters From One Region to a National Database.\",\"authors\":\"Justin Oake, Erfan Aref-Eshghi, Marshall Godwin, Kayla Collins, Kris Aubrey-Bassler, Pauline Duke, Masoud Mahdavian, Shabnam Asghari\",\"doi\":\"10.1177/1178222616685880\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>To assess the validity of the International Classification of Disease (ICD) codes for identifying patients with dyslipidemia in electronic medical record (EMR) data.</p><p><strong>Methods: </strong>The EMRs of patients receiving primary care in St. John's, Newfoundland and Labrador (NL), Canada, were retrieved from the Canadian Primary Care Sentinel Surveillance Network database. International Classification of Disease codes were first compared with laboratory lipid data as an independent criterion standard, and next with a \\\"comprehensive criterion standard,\\\" defined as any existence of abnormal lipid test, lipid-lowering medication record, or dyslipidemia ICD codes. The ability of ICD coding alone or combined with other components was evaluated against the two criterion standards using receiver operating characteristic (ROC) analysis, sensitivity, specificity, negative predictive value (NPV) and Kappa agreement. (No specificity was reported for the comparison of ICD codes against the comprehensive criterion standard as this naturally leads to 100% specificity.).</p><p><strong>Results: </strong>The ICD codes led to a poor outcome when compared with the serum lipid levels (sensitivity, 27%; specificity, 76%; PPV, 71%; NPV, 33%; Kappa, 0.02; area under the receiver operating characteristic curve (AUC), 0.51) or with the comprehensive criterion standard (sensitivity, 32%; NPV, 25%; Kappa, 0.15; AUC, 66%). International Classification of Disease codes combined with lipid-lowering medication data also resulted in low sensitivity (51.2%), NPV (32%), Kappa (0.28), and AUC (75%). The addition of laboratory lipid levels to ICD coding marginally improved the algorithm (sensitivity, 94%; NPV, 79%; Kappa, 0.85; AUC, 97%).</p><p><strong>Conclusions: </strong>The use of ICD coding, either alone or in combination with laboratory data or lipid-lowering medication records, was not an accurate indicator in identifying dyslipidemia.</p>\",\"PeriodicalId\":88397,\"journal\":{\"name\":\"Biomedical informatics insights\",\"volume\":\"9 \",\"pages\":\"1178222616685880\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2017-02-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1177/1178222616685880\",\"citationCount\":\"18\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Biomedical informatics insights\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/1178222616685880\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2017/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Biomedical informatics insights","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/1178222616685880","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2017/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Using Electronic Medical Record to Identify Patients With Dyslipidemia in Primary Care Settings: International Classification of Disease Code Matters From One Region to a National Database.
Objective: To assess the validity of the International Classification of Disease (ICD) codes for identifying patients with dyslipidemia in electronic medical record (EMR) data.
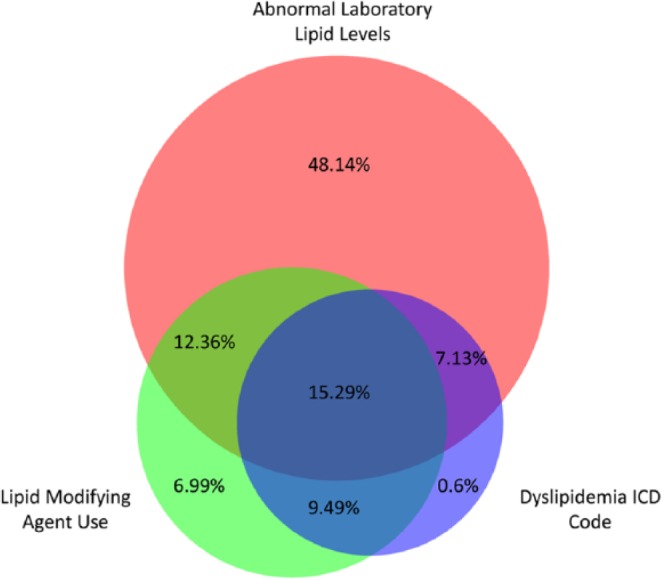
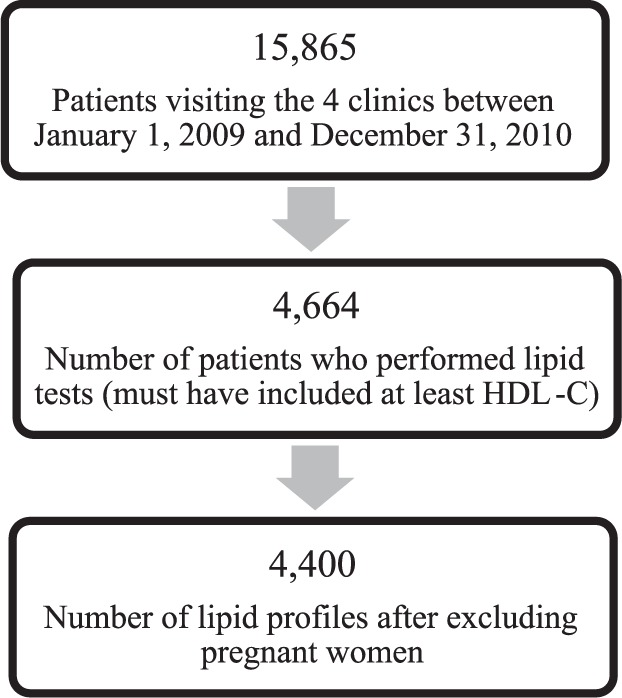
Methods: The EMRs of patients receiving primary care in St. John's, Newfoundland and Labrador (NL), Canada, were retrieved from the Canadian Primary Care Sentinel Surveillance Network database. International Classification of Disease codes were first compared with laboratory lipid data as an independent criterion standard, and next with a "comprehensive criterion standard," defined as any existence of abnormal lipid test, lipid-lowering medication record, or dyslipidemia ICD codes. The ability of ICD coding alone or combined with other components was evaluated against the two criterion standards using receiver operating characteristic (ROC) analysis, sensitivity, specificity, negative predictive value (NPV) and Kappa agreement. (No specificity was reported for the comparison of ICD codes against the comprehensive criterion standard as this naturally leads to 100% specificity.).
Results: The ICD codes led to a poor outcome when compared with the serum lipid levels (sensitivity, 27%; specificity, 76%; PPV, 71%; NPV, 33%; Kappa, 0.02; area under the receiver operating characteristic curve (AUC), 0.51) or with the comprehensive criterion standard (sensitivity, 32%; NPV, 25%; Kappa, 0.15; AUC, 66%). International Classification of Disease codes combined with lipid-lowering medication data also resulted in low sensitivity (51.2%), NPV (32%), Kappa (0.28), and AUC (75%). The addition of laboratory lipid levels to ICD coding marginally improved the algorithm (sensitivity, 94%; NPV, 79%; Kappa, 0.85; AUC, 97%).
Conclusions: The use of ICD coding, either alone or in combination with laboratory data or lipid-lowering medication records, was not an accurate indicator in identifying dyslipidemia.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


