Kudakwashe C Takarinda, Charles Sandy, Nyasha Masuka, Patrick Hazangwe, Regis C Choto, Tsitsi Mutasa-Apollo, Brilliant Nkomo, Edwin Sibanda, Owen Mugurungi, Anthony D Harries, Nicholas Siziba
{"title":"2013年津巴布韦南部地区接受结核病治疗的患者死亡率相关因素","authors":"Kudakwashe C Takarinda, Charles Sandy, Nyasha Masuka, Patrick Hazangwe, Regis C Choto, Tsitsi Mutasa-Apollo, Brilliant Nkomo, Edwin Sibanda, Owen Mugurungi, Anthony D Harries, Nicholas Siziba","doi":"10.1155/2017/6232071","DOIUrl":null,"url":null,"abstract":"<p><p><i>Background</i>. In 2013, the tuberculosis (TB) mortality rate was highest in southern Zimbabwe at 16%. We therefore sought to determine factors associated with mortality among registered TB patients in this region. <i>Methodology</i>. This was a retrospective record review of registered patients receiving anti-TB treatment in 2013. <i>Results</i>. Of 1,971 registered TB patients, 1,653 (84%) were new cases compared with 314 (16%) retreatment cases. There were 1,538 (78%) TB/human immunodeficiency virus (HIV) coinfected patients, of whom 1,399 (91%) were on antiretroviral therapy (ART) with median pre-ART CD4 count of 133 cells/uL (IQR, 46-282). Overall, 428 (22%) TB patients died. Factors associated with increased mortality included being ≥65 years old [adjusted relative risk (ARR) = 2.48 (95% CI 1.35-4.55)], a retreatment TB case [ARR = 1.34 (95% CI, 1.10-1.63)], and being HIV-positive [ARR = 1.87 (95% CI, 1.44-2.42)] whilst ART initiation was protective [ARR = 0.25 (95% CI, 0.22-0.29)]. Cumulative mortality rates were 10%, 14%, and 21% at one, two, and six months, respectively, after starting TB treatment. <i>Conclusion</i>. There was high mortality especially in the first two months of anti-TB treatment, with risk factors being recurrent TB and being HIV-infected, despite a high uptake of ART.</p>","PeriodicalId":30261,"journal":{"name":"Tuberculosis Research and Treatment","volume":"2017 ","pages":"6232071"},"PeriodicalIF":0.0000,"publicationDate":"2017-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5352882/pdf/","citationCount":"0","resultStr":"{\"title\":\"Factors Associated with Mortality among Patients on TB Treatment in the Southern Region of Zimbabwe, 2013.\",\"authors\":\"Kudakwashe C Takarinda, Charles Sandy, Nyasha Masuka, Patrick Hazangwe, Regis C Choto, Tsitsi Mutasa-Apollo, Brilliant Nkomo, Edwin Sibanda, Owen Mugurungi, Anthony D Harries, Nicholas Siziba\",\"doi\":\"10.1155/2017/6232071\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><i>Background</i>. In 2013, the tuberculosis (TB) mortality rate was highest in southern Zimbabwe at 16%. We therefore sought to determine factors associated with mortality among registered TB patients in this region. <i>Methodology</i>. This was a retrospective record review of registered patients receiving anti-TB treatment in 2013. <i>Results</i>. Of 1,971 registered TB patients, 1,653 (84%) were new cases compared with 314 (16%) retreatment cases. There were 1,538 (78%) TB/human immunodeficiency virus (HIV) coinfected patients, of whom 1,399 (91%) were on antiretroviral therapy (ART) with median pre-ART CD4 count of 133 cells/uL (IQR, 46-282). Overall, 428 (22%) TB patients died. Factors associated with increased mortality included being ≥65 years old [adjusted relative risk (ARR) = 2.48 (95% CI 1.35-4.55)], a retreatment TB case [ARR = 1.34 (95% CI, 1.10-1.63)], and being HIV-positive [ARR = 1.87 (95% CI, 1.44-2.42)] whilst ART initiation was protective [ARR = 0.25 (95% CI, 0.22-0.29)]. Cumulative mortality rates were 10%, 14%, and 21% at one, two, and six months, respectively, after starting TB treatment. <i>Conclusion</i>. There was high mortality especially in the first two months of anti-TB treatment, with risk factors being recurrent TB and being HIV-infected, despite a high uptake of ART.</p>\",\"PeriodicalId\":30261,\"journal\":{\"name\":\"Tuberculosis Research and Treatment\",\"volume\":\"2017 \",\"pages\":\"6232071\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2017-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5352882/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Tuberculosis Research and Treatment\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2017/6232071\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2017/3/2 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Tuberculosis Research and Treatment","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2017/6232071","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2017/3/2 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
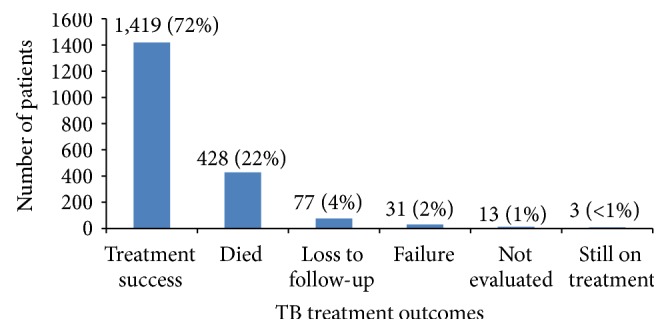
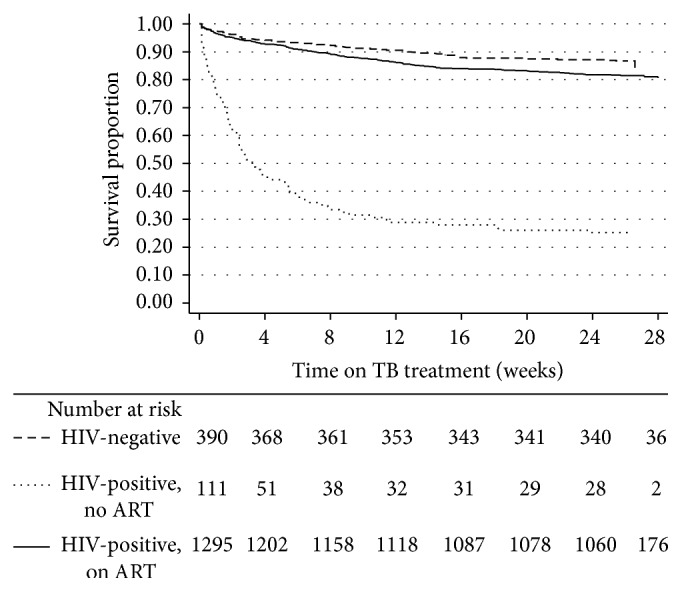
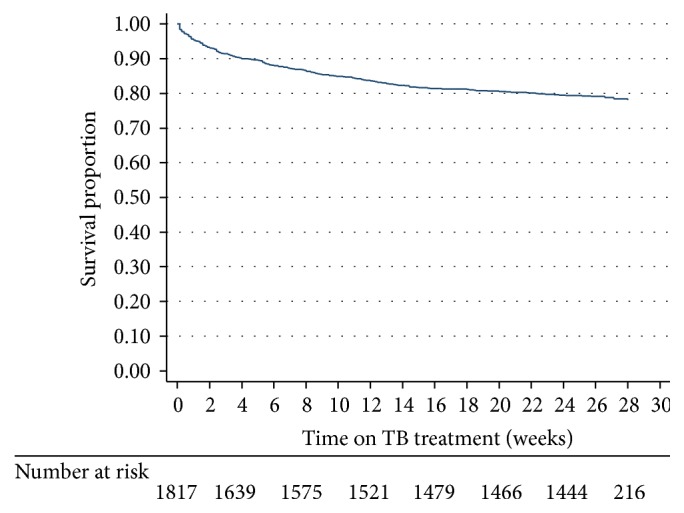
背景。2013年,津巴布韦南部的结核病死亡率最高,为16%。因此,我们试图确定与该地区登记结核病患者死亡率相关的因素。方法。这是对2013年接受抗结核治疗的注册患者的回顾性记录审查。结果。在1971名登记的结核病患者中,1653例(84%)为新发病例,314例(16%)为再治疗病例。共有1538例(78%)结核病/人类免疫缺陷病毒(HIV)合并感染患者,其中1399例(91%)接受抗逆转录病毒治疗(ART),抗逆转录病毒治疗前CD4细胞计数中位数为133细胞/uL (IQR, 46-282)。总体而言,428名(22%)结核病患者死亡。与死亡率增加相关的因素包括:年龄≥65岁[调整相对危险度(ARR) = 2.48 (95% CI 1.35-4.55)]、结核病再治疗病例[ARR = 1.34 (95% CI 1.10-1.63)]、hiv阳性[ARR = 1.87 (95% CI 1.44-2.42)],而开始抗逆转录病毒治疗具有保护作用[ARR = 0.25 (95% CI 0.22-0.29)]。在开始结核病治疗后1个月、2个月和6个月,累积死亡率分别为10%、14%和21%。结论。死亡率很高,特别是在抗结核治疗的头两个月,尽管抗逆转录病毒治疗的使用率很高,但危险因素是复发性结核病和感染艾滋病毒。
Factors Associated with Mortality among Patients on TB Treatment in the Southern Region of Zimbabwe, 2013.
Background. In 2013, the tuberculosis (TB) mortality rate was highest in southern Zimbabwe at 16%. We therefore sought to determine factors associated with mortality among registered TB patients in this region. Methodology. This was a retrospective record review of registered patients receiving anti-TB treatment in 2013. Results. Of 1,971 registered TB patients, 1,653 (84%) were new cases compared with 314 (16%) retreatment cases. There were 1,538 (78%) TB/human immunodeficiency virus (HIV) coinfected patients, of whom 1,399 (91%) were on antiretroviral therapy (ART) with median pre-ART CD4 count of 133 cells/uL (IQR, 46-282). Overall, 428 (22%) TB patients died. Factors associated with increased mortality included being ≥65 years old [adjusted relative risk (ARR) = 2.48 (95% CI 1.35-4.55)], a retreatment TB case [ARR = 1.34 (95% CI, 1.10-1.63)], and being HIV-positive [ARR = 1.87 (95% CI, 1.44-2.42)] whilst ART initiation was protective [ARR = 0.25 (95% CI, 0.22-0.29)]. Cumulative mortality rates were 10%, 14%, and 21% at one, two, and six months, respectively, after starting TB treatment. Conclusion. There was high mortality especially in the first two months of anti-TB treatment, with risk factors being recurrent TB and being HIV-infected, despite a high uptake of ART.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


