Jan Van Keer, David Derthoo, Olivier Van Caenegem, Michel De Pauw, Eric Nellessen, Nathalie Duerinckx, Walter Droogne, Gábor Vörös, Bart Meyns, Ann Belmans, Stefan Janssens, Johan Van Cleemput, Johan Vanhaecke
{"title":"CECARI研究:依维莫司(Certican®)起始和钙调磷酸酶抑制剂停药对肾功能不全的维护性心脏移植受者:一项多中心、随机试验。","authors":"Jan Van Keer, David Derthoo, Olivier Van Caenegem, Michel De Pauw, Eric Nellessen, Nathalie Duerinckx, Walter Droogne, Gábor Vörös, Bart Meyns, Ann Belmans, Stefan Janssens, Johan Van Cleemput, Johan Vanhaecke","doi":"10.1155/2017/6347138","DOIUrl":null,"url":null,"abstract":"<p><p>In this 3-year, open-label, multicenter study, 57 maintenance heart transplant recipients (>1 year after transplant) with renal insufficiency (eGFR 30-60 mL/min/1.73 m<sup>2</sup>) were randomized to start everolimus with CNI withdrawal (<i>N</i> = 29) or continue their current CNI-based immunosuppression (<i>N</i> = 28). The primary endpoint, change in measured glomerular filtration rate (mGFR) from baseline to year 3, did not differ significantly between both groups (+7.0 mL/min in the everolimus group versus +1.9 mL/min in the CNI group, <i>p</i> = 0.18). In the on-treatment analysis, the difference did reach statistical significance (+9.4 mL/min in the everolimus group versus +1.9 mL/min in the CNI group, <i>p</i> = 0.047). The composite safety endpoint of all-cause mortality, major adverse cardiovascular events, or treated acute rejection was not different between groups. Nonfatal adverse events occurred in 96.6% of patients in the everolimus group and 57.1% in the CNI group (<i>p</i> < 0.001). Ten patients (34.5%) in the everolimus group discontinued the study drug during follow-up due to adverse events. The poor adherence to the everolimus therapy might have masked a potential benefit of CNI withdrawal on renal function.</p>","PeriodicalId":45795,"journal":{"name":"Journal of Transplantation","volume":"2017 ","pages":"6347138"},"PeriodicalIF":2.2000,"publicationDate":"2017-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2017/6347138","citationCount":"7","resultStr":"{\"title\":\"The CECARI Study: Everolimus (Certican®) Initiation and Calcineurin Inhibitor Withdrawal in Maintenance Heart Transplant Recipients with Renal Insufficiency: A Multicenter, Randomized Trial.\",\"authors\":\"Jan Van Keer, David Derthoo, Olivier Van Caenegem, Michel De Pauw, Eric Nellessen, Nathalie Duerinckx, Walter Droogne, Gábor Vörös, Bart Meyns, Ann Belmans, Stefan Janssens, Johan Van Cleemput, Johan Vanhaecke\",\"doi\":\"10.1155/2017/6347138\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>In this 3-year, open-label, multicenter study, 57 maintenance heart transplant recipients (>1 year after transplant) with renal insufficiency (eGFR 30-60 mL/min/1.73 m<sup>2</sup>) were randomized to start everolimus with CNI withdrawal (<i>N</i> = 29) or continue their current CNI-based immunosuppression (<i>N</i> = 28). The primary endpoint, change in measured glomerular filtration rate (mGFR) from baseline to year 3, did not differ significantly between both groups (+7.0 mL/min in the everolimus group versus +1.9 mL/min in the CNI group, <i>p</i> = 0.18). In the on-treatment analysis, the difference did reach statistical significance (+9.4 mL/min in the everolimus group versus +1.9 mL/min in the CNI group, <i>p</i> = 0.047). The composite safety endpoint of all-cause mortality, major adverse cardiovascular events, or treated acute rejection was not different between groups. Nonfatal adverse events occurred in 96.6% of patients in the everolimus group and 57.1% in the CNI group (<i>p</i> < 0.001). Ten patients (34.5%) in the everolimus group discontinued the study drug during follow-up due to adverse events. The poor adherence to the everolimus therapy might have masked a potential benefit of CNI withdrawal on renal function.</p>\",\"PeriodicalId\":45795,\"journal\":{\"name\":\"Journal of Transplantation\",\"volume\":\"2017 \",\"pages\":\"6347138\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2017-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1155/2017/6347138\",\"citationCount\":\"7\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Transplantation\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2017/6347138\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2017/2/20 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Transplantation","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2017/6347138","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2017/2/20 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
The CECARI Study: Everolimus (Certican®) Initiation and Calcineurin Inhibitor Withdrawal in Maintenance Heart Transplant Recipients with Renal Insufficiency: A Multicenter, Randomized Trial.
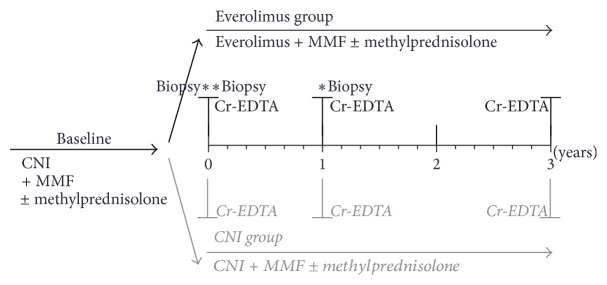
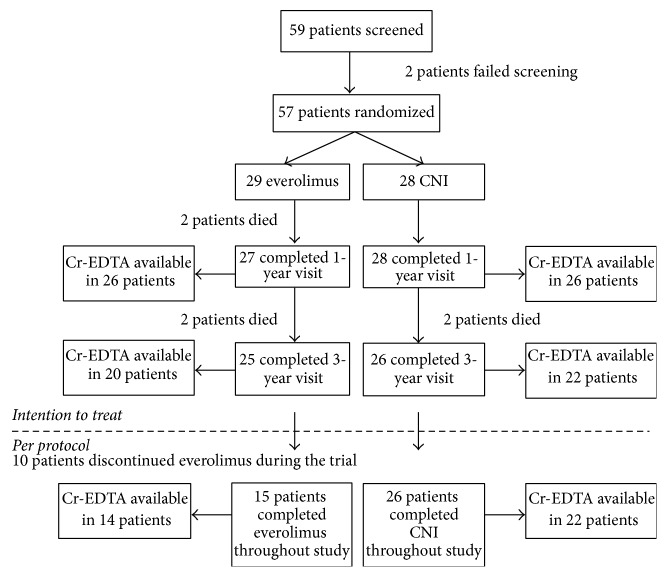
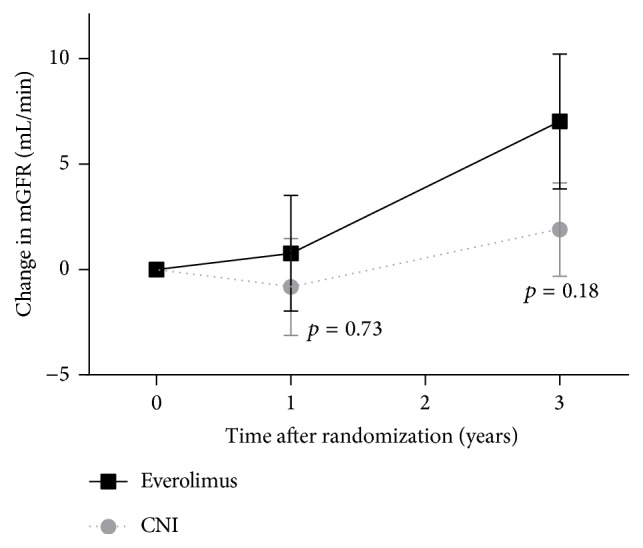
In this 3-year, open-label, multicenter study, 57 maintenance heart transplant recipients (>1 year after transplant) with renal insufficiency (eGFR 30-60 mL/min/1.73 m2) were randomized to start everolimus with CNI withdrawal (N = 29) or continue their current CNI-based immunosuppression (N = 28). The primary endpoint, change in measured glomerular filtration rate (mGFR) from baseline to year 3, did not differ significantly between both groups (+7.0 mL/min in the everolimus group versus +1.9 mL/min in the CNI group, p = 0.18). In the on-treatment analysis, the difference did reach statistical significance (+9.4 mL/min in the everolimus group versus +1.9 mL/min in the CNI group, p = 0.047). The composite safety endpoint of all-cause mortality, major adverse cardiovascular events, or treated acute rejection was not different between groups. Nonfatal adverse events occurred in 96.6% of patients in the everolimus group and 57.1% in the CNI group (p < 0.001). Ten patients (34.5%) in the everolimus group discontinued the study drug during follow-up due to adverse events. The poor adherence to the everolimus therapy might have masked a potential benefit of CNI withdrawal on renal function.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


