Rachel Spevack, Mohamed Al Shukairi, Dev Jayaraman, Jerrald Dankoff, Lawrence Rudski, Jed Lipes
{"title":"肺脏及下腔静脉超声在充血性心力衰竭评估中的应用。","authors":"Rachel Spevack, Mohamed Al Shukairi, Dev Jayaraman, Jerrald Dankoff, Lawrence Rudski, Jed Lipes","doi":"10.1186/s13089-017-0062-3","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Management of congestive heart failure (CHF) is dependent on clinical assessments of volume status, which are subjective and imprecise. Point-of-care ultrasound (POCUS) is useful in the diagnosis of CHF, but how POCUS findings correlate with therapy remains unknown. This study aimed to determine whether the changes in clinical evaluation of CHF with treatment are mirrored with changes in the number of B lines on lung ultrasound (LUS) and inferior vena cava (IVC) size. In this prospective observational study, investigators performed serial clinical and ultrasound assessments within 24 h of admission (T1), day 1 in hospital (T2) and within 24 h of discharge (T3). Clinical assessments included an evaluation of the jugular venous distension (JVD), hepatojugular reflux (HJR), pulmonary rales and a clinical congestion score was calculated. Ultrasound assessment included the IVC size and collapsibility, and the number of B lines in an 8-point scan.</p><p><strong>Results: </strong>Fifty consecutive patients were recruited with a mean age of 71.2 years (SD 12.7). Mean clinical congestion score on admission was 5.6 (SD 1.4) and declined significantly over time to 1.3 (0.91), as did the JVP, HJR and pulmonary rales. No significant changes were found in the IVC size between T1 [1.9 (0.65)] and T3 [2.0 (0.50)] or in the IVC collapsibility index [T1 0.3 (0.19) versus T3 0.25 (0.16)]. The mean number of B lines decreased from 11 (6.1) at T1 to 8.3 (5.5) at T3, although this decrease did not reach statistical significance. Spearman correlation between JVP and HJR versus IVC collapsibility and total B lines did not yield significant results.</p><p><strong>Conclusions: </strong>Clinical exam findings correlate over time during the management of CHF, whereas LUS and IVC results did not. The number of B lines did decrease with therapy, but did not reach statistical significance likely because the sampled population was small and had only mild heart failure. Further studies are warranted to further explore the use of lung ultrasound in this patient population.</p>","PeriodicalId":46598,"journal":{"name":"Critical Ultrasound Journal","volume":"9 1","pages":"7"},"PeriodicalIF":3.6000,"publicationDate":"2017-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/s13089-017-0062-3","citationCount":"22","resultStr":"{\"title\":\"Serial lung and IVC ultrasound in the assessment of congestive heart failure.\",\"authors\":\"Rachel Spevack, Mohamed Al Shukairi, Dev Jayaraman, Jerrald Dankoff, Lawrence Rudski, Jed Lipes\",\"doi\":\"10.1186/s13089-017-0062-3\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Management of congestive heart failure (CHF) is dependent on clinical assessments of volume status, which are subjective and imprecise. Point-of-care ultrasound (POCUS) is useful in the diagnosis of CHF, but how POCUS findings correlate with therapy remains unknown. This study aimed to determine whether the changes in clinical evaluation of CHF with treatment are mirrored with changes in the number of B lines on lung ultrasound (LUS) and inferior vena cava (IVC) size. In this prospective observational study, investigators performed serial clinical and ultrasound assessments within 24 h of admission (T1), day 1 in hospital (T2) and within 24 h of discharge (T3). Clinical assessments included an evaluation of the jugular venous distension (JVD), hepatojugular reflux (HJR), pulmonary rales and a clinical congestion score was calculated. Ultrasound assessment included the IVC size and collapsibility, and the number of B lines in an 8-point scan.</p><p><strong>Results: </strong>Fifty consecutive patients were recruited with a mean age of 71.2 years (SD 12.7). Mean clinical congestion score on admission was 5.6 (SD 1.4) and declined significantly over time to 1.3 (0.91), as did the JVP, HJR and pulmonary rales. No significant changes were found in the IVC size between T1 [1.9 (0.65)] and T3 [2.0 (0.50)] or in the IVC collapsibility index [T1 0.3 (0.19) versus T3 0.25 (0.16)]. The mean number of B lines decreased from 11 (6.1) at T1 to 8.3 (5.5) at T3, although this decrease did not reach statistical significance. Spearman correlation between JVP and HJR versus IVC collapsibility and total B lines did not yield significant results.</p><p><strong>Conclusions: </strong>Clinical exam findings correlate over time during the management of CHF, whereas LUS and IVC results did not. The number of B lines did decrease with therapy, but did not reach statistical significance likely because the sampled population was small and had only mild heart failure. Further studies are warranted to further explore the use of lung ultrasound in this patient population.</p>\",\"PeriodicalId\":46598,\"journal\":{\"name\":\"Critical Ultrasound Journal\",\"volume\":\"9 1\",\"pages\":\"7\"},\"PeriodicalIF\":3.6000,\"publicationDate\":\"2017-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1186/s13089-017-0062-3\",\"citationCount\":\"22\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Critical Ultrasound Journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s13089-017-0062-3\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2017/3/7 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical Ultrasound Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13089-017-0062-3","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2017/3/7 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
引用次数: 22
摘要
背景:充血性心力衰竭(CHF)的治疗依赖于容积状态的临床评估,这是主观的和不精确的。即时超声(POCUS)在诊断CHF中是有用的,但是POCUS的发现如何与治疗相关联仍然未知。本研究旨在确定治疗后CHF临床评价的变化是否反映在肺超声(LUS) B线数和下腔静脉(IVC)大小的变化上。在这项前瞻性观察性研究中,研究人员在入院24小时(T1)、入院第1天(T2)和出院24小时(T3)内进行了一系列临床和超声评估。临床评估包括颈静脉扩张(JVD)、肝颈静脉反流(HJR)、肺泡,并计算临床充血评分。超声评估包括下腔静脉的大小和可折叠性,以及8点扫描中B线的数量。结果:连续招募50例患者,平均年龄71.2岁(SD 12.7)。入院时的平均临床充血评分为5.6(标准差为1.4),随着时间的推移显著下降至1.3 (0.91),JVP、HJR和肺泡也是如此。在T1[1.9(0.65)]和T3[2.0(0.50)]之间,IVC大小没有显著变化,IVC可折叠性指数[T1 0.3 (0.19) vs T3 0.25(0.16)]也没有显著变化。B系平均数量由T1处理时的11株(6.1株)下降至T3处理时的8.3株(5.5株),但下降幅度无统计学意义。JVP和HJR与IVC溃散性和总B系的Spearman相关性没有显著结果。结论:临床检查结果与CHF治疗期间的时间相关,而LUS和IVC结果则不相关。B系的数量确实随着治疗而减少,但没有达到统计学意义,可能是因为采样人群很小,只有轻度心力衰竭。进一步的研究是必要的,以进一步探讨肺部超声在这一患者群体中的应用。
Serial lung and IVC ultrasound in the assessment of congestive heart failure.
Background: Management of congestive heart failure (CHF) is dependent on clinical assessments of volume status, which are subjective and imprecise. Point-of-care ultrasound (POCUS) is useful in the diagnosis of CHF, but how POCUS findings correlate with therapy remains unknown. This study aimed to determine whether the changes in clinical evaluation of CHF with treatment are mirrored with changes in the number of B lines on lung ultrasound (LUS) and inferior vena cava (IVC) size. In this prospective observational study, investigators performed serial clinical and ultrasound assessments within 24 h of admission (T1), day 1 in hospital (T2) and within 24 h of discharge (T3). Clinical assessments included an evaluation of the jugular venous distension (JVD), hepatojugular reflux (HJR), pulmonary rales and a clinical congestion score was calculated. Ultrasound assessment included the IVC size and collapsibility, and the number of B lines in an 8-point scan.
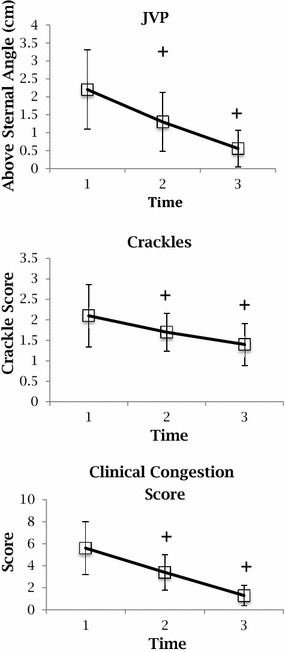
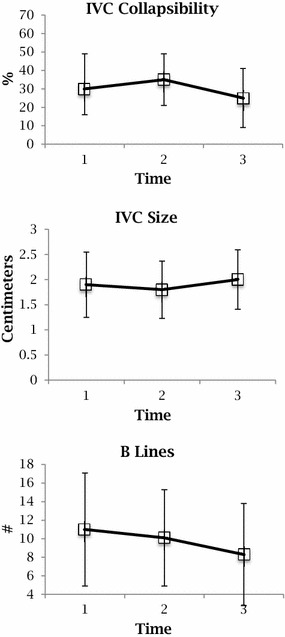
Results: Fifty consecutive patients were recruited with a mean age of 71.2 years (SD 12.7). Mean clinical congestion score on admission was 5.6 (SD 1.4) and declined significantly over time to 1.3 (0.91), as did the JVP, HJR and pulmonary rales. No significant changes were found in the IVC size between T1 [1.9 (0.65)] and T3 [2.0 (0.50)] or in the IVC collapsibility index [T1 0.3 (0.19) versus T3 0.25 (0.16)]. The mean number of B lines decreased from 11 (6.1) at T1 to 8.3 (5.5) at T3, although this decrease did not reach statistical significance. Spearman correlation between JVP and HJR versus IVC collapsibility and total B lines did not yield significant results.
Conclusions: Clinical exam findings correlate over time during the management of CHF, whereas LUS and IVC results did not. The number of B lines did decrease with therapy, but did not reach statistical significance likely because the sampled population was small and had only mild heart failure. Further studies are warranted to further explore the use of lung ultrasound in this patient population.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


