Mohamed Ghanem, Dirk Zajonz, Juliane Bollmann, Vanessa Geissler, Torsten Prietzel, Michael Moche, Andreas Roth, Christoph-E Heyde, Christoph Josten
{"title":"全膝关节置换术后骨水泥垫片治疗的疗效。","authors":"Mohamed Ghanem, Dirk Zajonz, Juliane Bollmann, Vanessa Geissler, Torsten Prietzel, Michael Moche, Andreas Roth, Christoph-E Heyde, Christoph Josten","doi":"10.3205/iprs000091","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Infection after total knee replacement (TKR) is one of the serious complications which must be pursued with a very effective therapeutic concept. In most cases this means revision arthroplasty, in which one-setting and two-setting procedures are distinguished. Healing of infection is the conditio sine qua non for re-implantation. This retrospective work presents an assessment of the success rate after a two-setting revision arthroplasty of the knee following periprosthetic infection. It further considers drawing conclusions concerning the optimal timing of re-implantation.</p><p><strong>Patients and methods: </strong>A total of 34 patients have been enclosed in this study from September 2005 to December 2013. 35 re-implantations were carried out following explantation of total knee and implantation of cemented spacer. The patient's group comprised of 53% (18) males and 47% (16) females. The average age at re-implantation time was 72.2 years (ranging from 54 to 85 years). We particularly evaluated the microbial spectrum, the interval between explantation and re-implantation, the number of surgeries that were necessary prior to re-implantation as well as the postoperative course.</p><p><strong>Results: </strong>We reported 31.4% (11) reinfections following re-implantation surgeries. The number of the reinfections declined with increasing time interval between explantation and re-implantation. Patients who developed reinfections were operated on (re-implantation) after an average of 4.47 months. Those patients with uncomplicated course were operated on (re-implantation) after an average of 6.79 months. Nevertheless, we noticed no essential differences in outcome with regard to the number of surgeries carried out prior to re-implantation. Mobile spacers proved better outcome than temporary arthrodesis with intramedullary fixation.</p><p><strong>Conclusion: </strong>No uniform strategy of treatment exists after peri-prosthetic infections. In particular, no optimal timing can be stated concerning re-implantation. Our data point out to the fact that a longer time interval between explantation and re-implantation reduces the rate of reinfection. From our point of view, the optimal timing for re-implantation depends on various specific factors and therefore it should be defined individually.</p>","PeriodicalId":43347,"journal":{"name":"GMS Interdisciplinary Plastic and Reconstructive Surgery DGPW","volume":"5 ","pages":"Doc12"},"PeriodicalIF":1.5000,"publicationDate":"2016-03-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4811200/pdf/","citationCount":"7","resultStr":"{\"title\":\"Outcome of total knee replacement following explantation and cemented spacer therapy.\",\"authors\":\"Mohamed Ghanem, Dirk Zajonz, Juliane Bollmann, Vanessa Geissler, Torsten Prietzel, Michael Moche, Andreas Roth, Christoph-E Heyde, Christoph Josten\",\"doi\":\"10.3205/iprs000091\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Infection after total knee replacement (TKR) is one of the serious complications which must be pursued with a very effective therapeutic concept. In most cases this means revision arthroplasty, in which one-setting and two-setting procedures are distinguished. Healing of infection is the conditio sine qua non for re-implantation. This retrospective work presents an assessment of the success rate after a two-setting revision arthroplasty of the knee following periprosthetic infection. It further considers drawing conclusions concerning the optimal timing of re-implantation.</p><p><strong>Patients and methods: </strong>A total of 34 patients have been enclosed in this study from September 2005 to December 2013. 35 re-implantations were carried out following explantation of total knee and implantation of cemented spacer. The patient's group comprised of 53% (18) males and 47% (16) females. The average age at re-implantation time was 72.2 years (ranging from 54 to 85 years). We particularly evaluated the microbial spectrum, the interval between explantation and re-implantation, the number of surgeries that were necessary prior to re-implantation as well as the postoperative course.</p><p><strong>Results: </strong>We reported 31.4% (11) reinfections following re-implantation surgeries. The number of the reinfections declined with increasing time interval between explantation and re-implantation. Patients who developed reinfections were operated on (re-implantation) after an average of 4.47 months. Those patients with uncomplicated course were operated on (re-implantation) after an average of 6.79 months. Nevertheless, we noticed no essential differences in outcome with regard to the number of surgeries carried out prior to re-implantation. Mobile spacers proved better outcome than temporary arthrodesis with intramedullary fixation.</p><p><strong>Conclusion: </strong>No uniform strategy of treatment exists after peri-prosthetic infections. In particular, no optimal timing can be stated concerning re-implantation. Our data point out to the fact that a longer time interval between explantation and re-implantation reduces the rate of reinfection. From our point of view, the optimal timing for re-implantation depends on various specific factors and therefore it should be defined individually.</p>\",\"PeriodicalId\":43347,\"journal\":{\"name\":\"GMS Interdisciplinary Plastic and Reconstructive Surgery DGPW\",\"volume\":\"5 \",\"pages\":\"Doc12\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2016-03-24\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4811200/pdf/\",\"citationCount\":\"7\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"GMS Interdisciplinary Plastic and Reconstructive Surgery DGPW\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3205/iprs000091\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2016/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"GMS Interdisciplinary Plastic and Reconstructive Surgery DGPW","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3205/iprs000091","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2016/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
Outcome of total knee replacement following explantation and cemented spacer therapy.
Background: Infection after total knee replacement (TKR) is one of the serious complications which must be pursued with a very effective therapeutic concept. In most cases this means revision arthroplasty, in which one-setting and two-setting procedures are distinguished. Healing of infection is the conditio sine qua non for re-implantation. This retrospective work presents an assessment of the success rate after a two-setting revision arthroplasty of the knee following periprosthetic infection. It further considers drawing conclusions concerning the optimal timing of re-implantation.
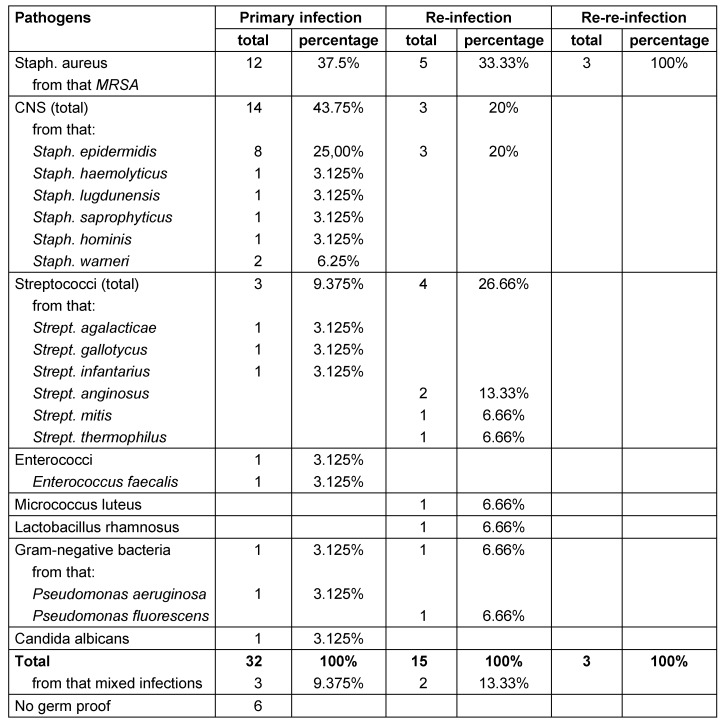
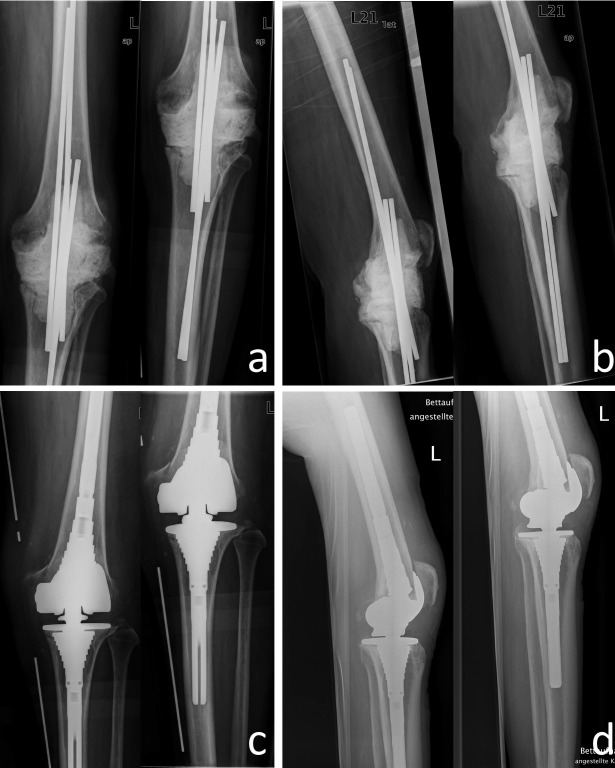
Patients and methods: A total of 34 patients have been enclosed in this study from September 2005 to December 2013. 35 re-implantations were carried out following explantation of total knee and implantation of cemented spacer. The patient's group comprised of 53% (18) males and 47% (16) females. The average age at re-implantation time was 72.2 years (ranging from 54 to 85 years). We particularly evaluated the microbial spectrum, the interval between explantation and re-implantation, the number of surgeries that were necessary prior to re-implantation as well as the postoperative course.
Results: We reported 31.4% (11) reinfections following re-implantation surgeries. The number of the reinfections declined with increasing time interval between explantation and re-implantation. Patients who developed reinfections were operated on (re-implantation) after an average of 4.47 months. Those patients with uncomplicated course were operated on (re-implantation) after an average of 6.79 months. Nevertheless, we noticed no essential differences in outcome with regard to the number of surgeries carried out prior to re-implantation. Mobile spacers proved better outcome than temporary arthrodesis with intramedullary fixation.
Conclusion: No uniform strategy of treatment exists after peri-prosthetic infections. In particular, no optimal timing can be stated concerning re-implantation. Our data point out to the fact that a longer time interval between explantation and re-implantation reduces the rate of reinfection. From our point of view, the optimal timing for re-implantation depends on various specific factors and therefore it should be defined individually.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


