{"title":"免疫性血小板减少症的诊断和治疗进展。","authors":"Shosaku Nomura","doi":"10.4137/CMBD.S39643","DOIUrl":null,"url":null,"abstract":"<p><p>Immune thrombocytopenia (ITP) is an acquired hemorrhagic condition characterized by the accelerated clearance of platelets caused by antiplatelet autoantibodies. A platelet count in peripheral blood <100 × 10(9)/L is the most important criterion for the diagnosis of ITP. However, the platelet count is not the sole diagnostic criterion, and the diagnosis of ITP is dependent on additional findings. ITP can be classified into three types, namely, acute, subchronic, and persistent, based on disease duration. Conventional therapy includes corticosteroids, intravenous immunoglobulin, splenectomy, and watch-and-wait. Second-line treatments for ITP include immunosuppressive therapy [eg, anti-CD20 (rituximab)], with international guidelines, including rituximab as a second-line option. The most recently licensed drugs for ITP are the thrombopoietin receptor agonists (TRAs), such as romiplostim and eltrombopag. TRAs are associated with increased platelet counts and reductions in the number of bleeding events. TRAs are usually considered safe, effective treatments for patients with chronic ITP at risk of bleeding after failure of first-line therapies. Due to the high costs of TRAs, however, it is unclear if patients prefer these agents. In addition, some new agents are under development now. This manuscript summarizes the pathophysiology, diagnosis, and treatment of ITP. The goal of all treatment strategies for ITP is to achieve a platelet count that is associated with adequate hemostasis, rather than a normal platelet count. The decision to treat should be based on the bleeding severity, bleeding risk, activity level, likely side effects of treatment, and patient preferences. </p>","PeriodicalId":43083,"journal":{"name":"Clinical Medicine Insights-Blood Disorders","volume":"9 ","pages":"15-22"},"PeriodicalIF":3.0000,"publicationDate":"2016-07-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.4137/CMBD.S39643","citationCount":"53","resultStr":"{\"title\":\"Advances in Diagnosis and Treatments for Immune Thrombocytopenia.\",\"authors\":\"Shosaku Nomura\",\"doi\":\"10.4137/CMBD.S39643\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Immune thrombocytopenia (ITP) is an acquired hemorrhagic condition characterized by the accelerated clearance of platelets caused by antiplatelet autoantibodies. A platelet count in peripheral blood <100 × 10(9)/L is the most important criterion for the diagnosis of ITP. However, the platelet count is not the sole diagnostic criterion, and the diagnosis of ITP is dependent on additional findings. ITP can be classified into three types, namely, acute, subchronic, and persistent, based on disease duration. Conventional therapy includes corticosteroids, intravenous immunoglobulin, splenectomy, and watch-and-wait. Second-line treatments for ITP include immunosuppressive therapy [eg, anti-CD20 (rituximab)], with international guidelines, including rituximab as a second-line option. The most recently licensed drugs for ITP are the thrombopoietin receptor agonists (TRAs), such as romiplostim and eltrombopag. TRAs are associated with increased platelet counts and reductions in the number of bleeding events. TRAs are usually considered safe, effective treatments for patients with chronic ITP at risk of bleeding after failure of first-line therapies. Due to the high costs of TRAs, however, it is unclear if patients prefer these agents. In addition, some new agents are under development now. This manuscript summarizes the pathophysiology, diagnosis, and treatment of ITP. The goal of all treatment strategies for ITP is to achieve a platelet count that is associated with adequate hemostasis, rather than a normal platelet count. The decision to treat should be based on the bleeding severity, bleeding risk, activity level, likely side effects of treatment, and patient preferences. </p>\",\"PeriodicalId\":43083,\"journal\":{\"name\":\"Clinical Medicine Insights-Blood Disorders\",\"volume\":\"9 \",\"pages\":\"15-22\"},\"PeriodicalIF\":3.0000,\"publicationDate\":\"2016-07-17\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.4137/CMBD.S39643\",\"citationCount\":\"53\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Medicine Insights-Blood Disorders\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4137/CMBD.S39643\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2016/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine Insights-Blood Disorders","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4137/CMBD.S39643","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2016/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
Advances in Diagnosis and Treatments for Immune Thrombocytopenia.
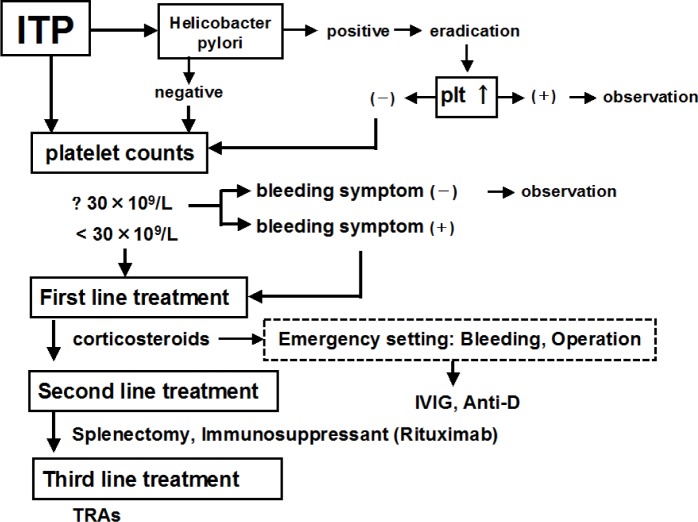
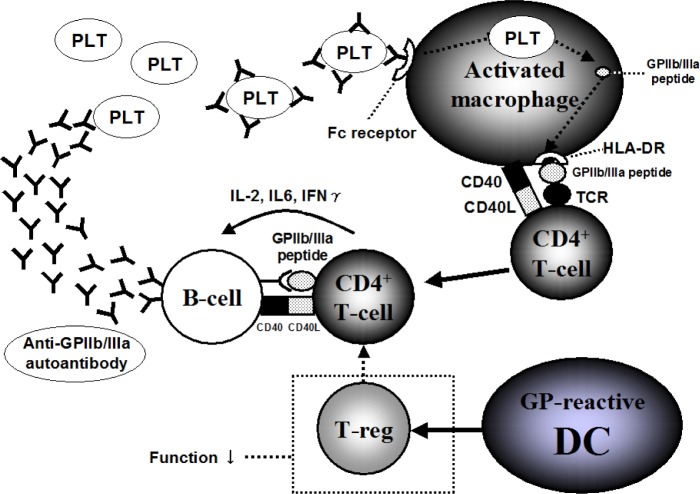
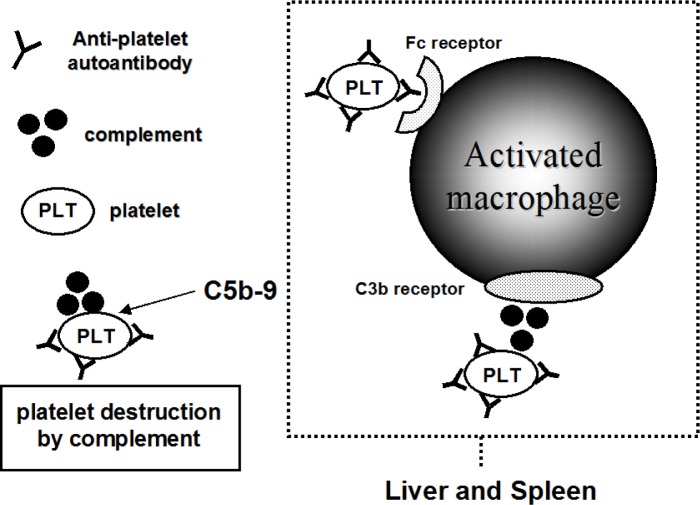
Immune thrombocytopenia (ITP) is an acquired hemorrhagic condition characterized by the accelerated clearance of platelets caused by antiplatelet autoantibodies. A platelet count in peripheral blood <100 × 10(9)/L is the most important criterion for the diagnosis of ITP. However, the platelet count is not the sole diagnostic criterion, and the diagnosis of ITP is dependent on additional findings. ITP can be classified into three types, namely, acute, subchronic, and persistent, based on disease duration. Conventional therapy includes corticosteroids, intravenous immunoglobulin, splenectomy, and watch-and-wait. Second-line treatments for ITP include immunosuppressive therapy [eg, anti-CD20 (rituximab)], with international guidelines, including rituximab as a second-line option. The most recently licensed drugs for ITP are the thrombopoietin receptor agonists (TRAs), such as romiplostim and eltrombopag. TRAs are associated with increased platelet counts and reductions in the number of bleeding events. TRAs are usually considered safe, effective treatments for patients with chronic ITP at risk of bleeding after failure of first-line therapies. Due to the high costs of TRAs, however, it is unclear if patients prefer these agents. In addition, some new agents are under development now. This manuscript summarizes the pathophysiology, diagnosis, and treatment of ITP. The goal of all treatment strategies for ITP is to achieve a platelet count that is associated with adequate hemostasis, rather than a normal platelet count. The decision to treat should be based on the bleeding severity, bleeding risk, activity level, likely side effects of treatment, and patient preferences.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


