Dong-Hyun Lee, Kyoung-Tae Kim, Jeong-Ill Park, Ki-Su Park, Dae-Chul Cho, Joo-Kyung Sung
{"title":"双层硬脑膜成形术修复胸椎难以触及的硬脑膜腹侧缺损。","authors":"Dong-Hyun Lee, Kyoung-Tae Kim, Jeong-Ill Park, Ki-Su Park, Dae-Chul Cho, Joo-Kyung Sung","doi":"10.14245/kjs.2016.13.2.87","DOIUrl":null,"url":null,"abstract":"<p><p>We propose a double layered (intradural and epidural patch) duraplasty that utilizes Lyoplant and Duraseal. We examined a 47-year-old woman after decompression for thoracic ossification of posterior longitudinal ligament was performed in another hospital. On postoperative day 7, she complained of weakness in both legs. Postoperative magnetic resonance imaging (MRI) showed cerebrospinal fluid (CSF) collection with cord compression. In the operative field, we found 2 large dural defects on the ventral dura mater. We performed a conventional fat graft with fibrin glue. However, the patient exhibited neurologic deterioration, and a postoperative MRI again showed CSF collection. We performed dorsal midline durotomy and inserted a intradural and epidural Lyoplant patch. She immediately experienced diminishing back pain postoperatively. Her visual analog scale and motor power improved markedly. Postoperative MRIs performed at 2 and 16 months showed no spinal cord compression or CSF leakage to the epidural space. We describe a new technique for double layered duraplasty. Although we do not recommend this technique for all dural repairs, double-layered duraplasty may be useful for repairing large inaccessible dural tears in cases of persistent CSF leakage refractory to conventional management. </p>","PeriodicalId":17867,"journal":{"name":"Korean Journal of Spine","volume":"13 2","pages":"87-90"},"PeriodicalIF":0.0000,"publicationDate":"2016-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ef/f4/kjs-13-87.PMC4949176.pdf","citationCount":"10","resultStr":"{\"title\":\"Repair of Inaccessible Ventral Dural Defect in Thoracic Spine: Double Layered Duraplasty.\",\"authors\":\"Dong-Hyun Lee, Kyoung-Tae Kim, Jeong-Ill Park, Ki-Su Park, Dae-Chul Cho, Joo-Kyung Sung\",\"doi\":\"10.14245/kjs.2016.13.2.87\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>We propose a double layered (intradural and epidural patch) duraplasty that utilizes Lyoplant and Duraseal. We examined a 47-year-old woman after decompression for thoracic ossification of posterior longitudinal ligament was performed in another hospital. On postoperative day 7, she complained of weakness in both legs. Postoperative magnetic resonance imaging (MRI) showed cerebrospinal fluid (CSF) collection with cord compression. In the operative field, we found 2 large dural defects on the ventral dura mater. We performed a conventional fat graft with fibrin glue. However, the patient exhibited neurologic deterioration, and a postoperative MRI again showed CSF collection. We performed dorsal midline durotomy and inserted a intradural and epidural Lyoplant patch. She immediately experienced diminishing back pain postoperatively. Her visual analog scale and motor power improved markedly. Postoperative MRIs performed at 2 and 16 months showed no spinal cord compression or CSF leakage to the epidural space. We describe a new technique for double layered duraplasty. Although we do not recommend this technique for all dural repairs, double-layered duraplasty may be useful for repairing large inaccessible dural tears in cases of persistent CSF leakage refractory to conventional management. </p>\",\"PeriodicalId\":17867,\"journal\":{\"name\":\"Korean Journal of Spine\",\"volume\":\"13 2\",\"pages\":\"87-90\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2016-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ef/f4/kjs-13-87.PMC4949176.pdf\",\"citationCount\":\"10\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Korean Journal of Spine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14245/kjs.2016.13.2.87\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2016/6/30 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Korean Journal of Spine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14245/kjs.2016.13.2.87","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2016/6/30 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Repair of Inaccessible Ventral Dural Defect in Thoracic Spine: Double Layered Duraplasty.
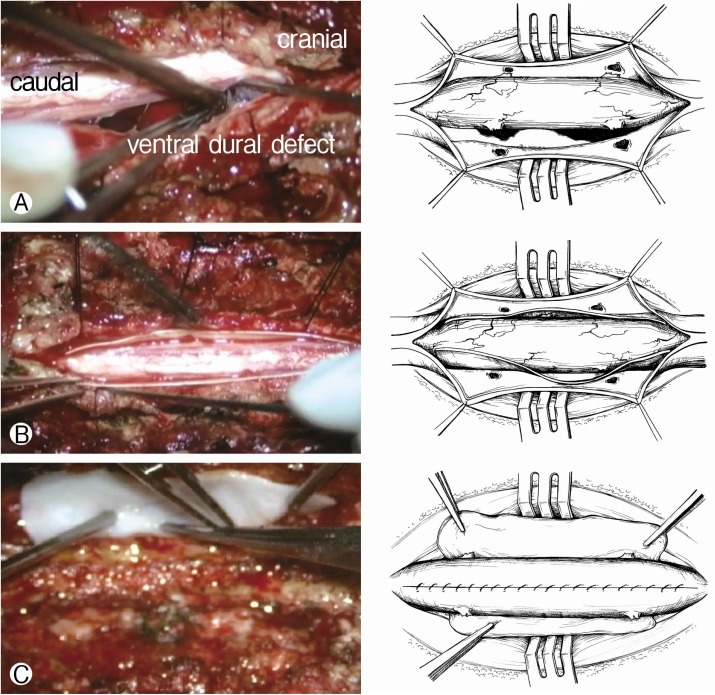
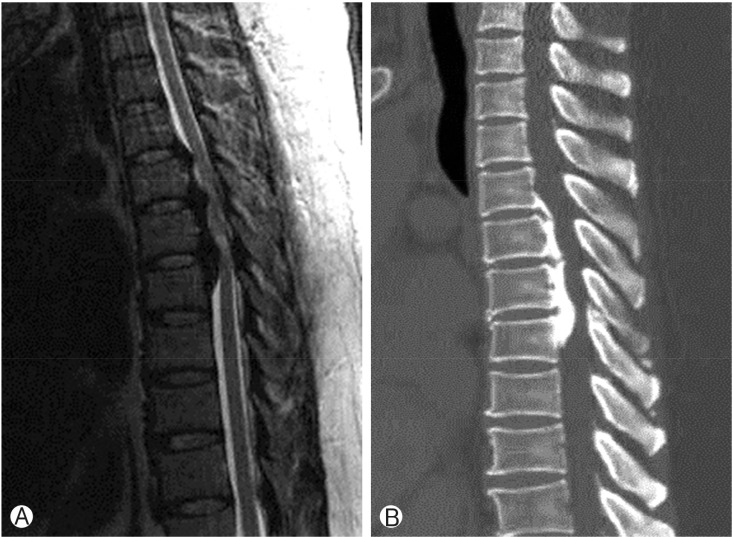
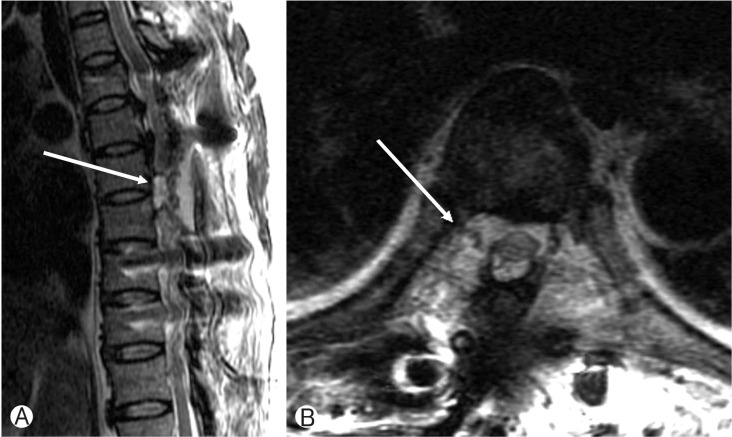
We propose a double layered (intradural and epidural patch) duraplasty that utilizes Lyoplant and Duraseal. We examined a 47-year-old woman after decompression for thoracic ossification of posterior longitudinal ligament was performed in another hospital. On postoperative day 7, she complained of weakness in both legs. Postoperative magnetic resonance imaging (MRI) showed cerebrospinal fluid (CSF) collection with cord compression. In the operative field, we found 2 large dural defects on the ventral dura mater. We performed a conventional fat graft with fibrin glue. However, the patient exhibited neurologic deterioration, and a postoperative MRI again showed CSF collection. We performed dorsal midline durotomy and inserted a intradural and epidural Lyoplant patch. She immediately experienced diminishing back pain postoperatively. Her visual analog scale and motor power improved markedly. Postoperative MRIs performed at 2 and 16 months showed no spinal cord compression or CSF leakage to the epidural space. We describe a new technique for double layered duraplasty. Although we do not recommend this technique for all dural repairs, double-layered duraplasty may be useful for repairing large inaccessible dural tears in cases of persistent CSF leakage refractory to conventional management.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


