Rohan Gupta, Neda Heshami, Chouhan Jay, Naveen Ramesh, Juhee Song, Xiudong Lei, Erfe Jean Rose, Kristen Carter, Dejka M Araujo, Robert S Benjamin, Shreyaskumar Patel, Joseph L Nates, Vinod Ravi
{"title":"入住重症监护病房的肉瘤患者的生存预测因素。","authors":"Rohan Gupta, Neda Heshami, Chouhan Jay, Naveen Ramesh, Juhee Song, Xiudong Lei, Erfe Jean Rose, Kristen Carter, Dejka M Araujo, Robert S Benjamin, Shreyaskumar Patel, Joseph L Nates, Vinod Ravi","doi":"10.1186/s13569-016-0051-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Advances in treatment of sarcoma patients has prolonged survival but has led to increased disease- or treatment-related complications resulting in greater number of admissions to the intensive care unit (ICU). Survival and long-term outcome information about such critically ill patients with sarcoma is unknown.</p><p><strong>Methods: </strong>The primary objective of the study was to determine the ICU and post-ICU survival rates of critically ill sarcoma patients. Secondary objectives included determining the modifiable and non-modifiable predictors of poor survival. We performed a retrospective chart review of sarcoma patients admitted to the ICU at The University of Texas MD Anderson Cancer Center between January 1, 2005, and December 31, 2012. Main outcome measures were ICU mortality, in-hospital mortality and 1, 2, and 6-month survival rates. Covariates such as histological diagnosis, disease characteristics, chemotherapy use, Charlson comorbidity index, Sequential Organ Failure Assessment (SOFA) scores, and clinical findings leading to ICU admission were analyzed for their effects on survival.</p><p><strong>Results: </strong>We identified 172 admissions over the 8-year study period hat met our inclusion criteria. The study population was 45.9 % males with a median age of 52 years. The most common sarcoma subgroups were high-grade unclassified sarcoma (25 %) and bone tumors (17.4 %). The ICU mortality rate was 23.3 % (95 % confidence interval [CI], 16.9-29.6 %), and an additional 6.4 % of patients died before hospital discharge (95 % CI, 22.9-37.1 %). 6-month OS rates were 41 %. The median SOFA scores on admission were 6 (inter quartile range (IQR), 3.5-9) in ICU survivors and 10 (IQR, 6.5-14) in ICU non-survivors. Increase in SOFA scores ≥6 led to poor outcomes (ICU survival 13.3 %, OS 6.7 %). Charlson comorbidity index (HR 1.139, 95 % CI 1.023-1.268, p = 0.02) and discharge SOFA scores (HR 1.210, 95 % CI 1.141-1.283, p < 0.0001) correlated with overall survival.</p><p><strong>Conclusions: </strong>Our results suggest that patients that are admitted to the ICU for respiratory failure, cardiac arrest, septic shock, acute renal failure or acidosis and also have a high SOFA score with subsequent worsening in the ICU have poor prognosis. Based on the retrospective data which needs further validation we can recommend that judicious approach should be taken in patients with predictors of poor survival before subjecting them to aggressive treatment.</p>","PeriodicalId":10684,"journal":{"name":"Clinical Sarcoma Research","volume":"6 ","pages":"12"},"PeriodicalIF":0.0000,"publicationDate":"2016-07-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/s13569-016-0051-5","citationCount":"5","resultStr":"{\"title\":\"Predictors of survival in patients with sarcoma admitted to the intensive care unit.\",\"authors\":\"Rohan Gupta, Neda Heshami, Chouhan Jay, Naveen Ramesh, Juhee Song, Xiudong Lei, Erfe Jean Rose, Kristen Carter, Dejka M Araujo, Robert S Benjamin, Shreyaskumar Patel, Joseph L Nates, Vinod Ravi\",\"doi\":\"10.1186/s13569-016-0051-5\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Advances in treatment of sarcoma patients has prolonged survival but has led to increased disease- or treatment-related complications resulting in greater number of admissions to the intensive care unit (ICU). Survival and long-term outcome information about such critically ill patients with sarcoma is unknown.</p><p><strong>Methods: </strong>The primary objective of the study was to determine the ICU and post-ICU survival rates of critically ill sarcoma patients. Secondary objectives included determining the modifiable and non-modifiable predictors of poor survival. We performed a retrospective chart review of sarcoma patients admitted to the ICU at The University of Texas MD Anderson Cancer Center between January 1, 2005, and December 31, 2012. Main outcome measures were ICU mortality, in-hospital mortality and 1, 2, and 6-month survival rates. Covariates such as histological diagnosis, disease characteristics, chemotherapy use, Charlson comorbidity index, Sequential Organ Failure Assessment (SOFA) scores, and clinical findings leading to ICU admission were analyzed for their effects on survival.</p><p><strong>Results: </strong>We identified 172 admissions over the 8-year study period hat met our inclusion criteria. The study population was 45.9 % males with a median age of 52 years. The most common sarcoma subgroups were high-grade unclassified sarcoma (25 %) and bone tumors (17.4 %). The ICU mortality rate was 23.3 % (95 % confidence interval [CI], 16.9-29.6 %), and an additional 6.4 % of patients died before hospital discharge (95 % CI, 22.9-37.1 %). 6-month OS rates were 41 %. The median SOFA scores on admission were 6 (inter quartile range (IQR), 3.5-9) in ICU survivors and 10 (IQR, 6.5-14) in ICU non-survivors. Increase in SOFA scores ≥6 led to poor outcomes (ICU survival 13.3 %, OS 6.7 %). Charlson comorbidity index (HR 1.139, 95 % CI 1.023-1.268, p = 0.02) and discharge SOFA scores (HR 1.210, 95 % CI 1.141-1.283, p < 0.0001) correlated with overall survival.</p><p><strong>Conclusions: </strong>Our results suggest that patients that are admitted to the ICU for respiratory failure, cardiac arrest, septic shock, acute renal failure or acidosis and also have a high SOFA score with subsequent worsening in the ICU have poor prognosis. Based on the retrospective data which needs further validation we can recommend that judicious approach should be taken in patients with predictors of poor survival before subjecting them to aggressive treatment.</p>\",\"PeriodicalId\":10684,\"journal\":{\"name\":\"Clinical Sarcoma Research\",\"volume\":\"6 \",\"pages\":\"12\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2016-07-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1186/s13569-016-0051-5\",\"citationCount\":\"5\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Sarcoma Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s13569-016-0051-5\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2016/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Sarcoma Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13569-016-0051-5","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2016/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 5
摘要
背景:肉瘤治疗的进步延长了患者的生存期,但也导致了疾病或治疗相关并发症的增加,导致更多的患者入住重症监护病房(ICU)。这些危重肉瘤患者的生存和长期预后信息尚不清楚。方法:研究的主要目的是确定危重期肉瘤患者的ICU和ICU后生存率。次要目标包括确定不良生存的可修改和不可修改的预测因素。我们对2005年1月1日至2012年12月31日期间在德克萨斯大学MD安德森癌症中心ICU收治的肉瘤患者进行了回顾性图表回顾。主要结局指标为ICU死亡率、住院死亡率和1、2、6个月生存率。协变量如组织学诊断、疾病特征、化疗使用、Charlson合并症指数、序贯器官衰竭评估(SOFA)评分和导致ICU入院的临床表现对生存的影响进行了分析。结果:在8年的研究期间,我们确定了172例符合纳入标准的入院患者。研究人群中45.9%为男性,中位年龄52岁。最常见的肉瘤亚组是高级别未分类肉瘤(25%)和骨肿瘤(17.4%)。ICU死亡率为23.3%(95%可信区间[CI], 16.9 ~ 29.6%),另有6.4%的患者在出院前死亡(95% CI, 22.9 ~ 37.1%)。6个月的OS率为41%。ICU存活者入院时SOFA评分中位数为6分(四分位间距(IQR), 3.5-9分),非ICU存活者为10分(IQR, 6.5-14分)。SOFA评分≥6导致预后不良(ICU生存率13.3%,OS为6.7%)。Charlson合并症指数(HR 1.139, 95% CI 1.023-1.268, p = 0.02)和出院时SOFA评分(HR 1.210, 95% CI 1.141-1.283, p)结论:因呼吸衰竭、心脏骤停、感染性休克、急性肾功能衰竭或酸中毒而入住ICU且SOFA评分较高且随后恶化的患者预后较差。根据需要进一步验证的回顾性数据,我们可以建议在对预后不良的患者进行积极治疗之前,应采取明智的方法。
Predictors of survival in patients with sarcoma admitted to the intensive care unit.
Background: Advances in treatment of sarcoma patients has prolonged survival but has led to increased disease- or treatment-related complications resulting in greater number of admissions to the intensive care unit (ICU). Survival and long-term outcome information about such critically ill patients with sarcoma is unknown.
Methods: The primary objective of the study was to determine the ICU and post-ICU survival rates of critically ill sarcoma patients. Secondary objectives included determining the modifiable and non-modifiable predictors of poor survival. We performed a retrospective chart review of sarcoma patients admitted to the ICU at The University of Texas MD Anderson Cancer Center between January 1, 2005, and December 31, 2012. Main outcome measures were ICU mortality, in-hospital mortality and 1, 2, and 6-month survival rates. Covariates such as histological diagnosis, disease characteristics, chemotherapy use, Charlson comorbidity index, Sequential Organ Failure Assessment (SOFA) scores, and clinical findings leading to ICU admission were analyzed for their effects on survival.
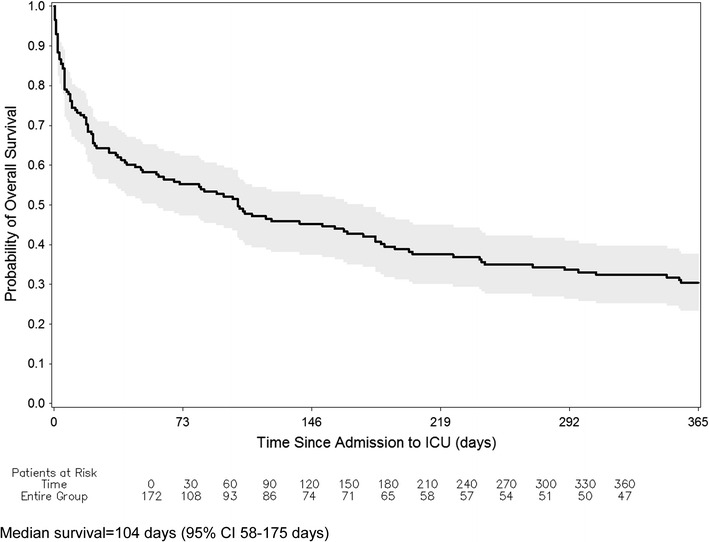
Results: We identified 172 admissions over the 8-year study period hat met our inclusion criteria. The study population was 45.9 % males with a median age of 52 years. The most common sarcoma subgroups were high-grade unclassified sarcoma (25 %) and bone tumors (17.4 %). The ICU mortality rate was 23.3 % (95 % confidence interval [CI], 16.9-29.6 %), and an additional 6.4 % of patients died before hospital discharge (95 % CI, 22.9-37.1 %). 6-month OS rates were 41 %. The median SOFA scores on admission were 6 (inter quartile range (IQR), 3.5-9) in ICU survivors and 10 (IQR, 6.5-14) in ICU non-survivors. Increase in SOFA scores ≥6 led to poor outcomes (ICU survival 13.3 %, OS 6.7 %). Charlson comorbidity index (HR 1.139, 95 % CI 1.023-1.268, p = 0.02) and discharge SOFA scores (HR 1.210, 95 % CI 1.141-1.283, p < 0.0001) correlated with overall survival.
Conclusions: Our results suggest that patients that are admitted to the ICU for respiratory failure, cardiac arrest, septic shock, acute renal failure or acidosis and also have a high SOFA score with subsequent worsening in the ICU have poor prognosis. Based on the retrospective data which needs further validation we can recommend that judicious approach should be taken in patients with predictors of poor survival before subjecting them to aggressive treatment.
期刊介绍:
Clinical Sarcoma Research considers for publication articles related to research on sarcomas, including both soft tissue and bone. The journal publishes original articles and review articles on the diagnosis and treatment of sarcomas along with new insights in sarcoma research, which may be of immediate or future interest for diagnosis and treatment. The journal also considers negative results, especially those from studies on new agents, as it is vital for the medical community to learn whether new agents have been proven effective or ineffective within subtypes of sarcomas. The journal also aims to offer a forum for active discussion on topics of major interest for the sarcoma community, which may be related to both research results and methodological topics.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


