Sushanta K Sahoo, Arsikere N Deepak, Pravin Salunke
{"title":"成人拉森综合征伴寰枢关节脱位后凸畸形1例。","authors":"Sushanta K Sahoo, Arsikere N Deepak, Pravin Salunke","doi":"10.4103/0974-8237.181869","DOIUrl":null,"url":null,"abstract":"<p><p>Kyphotic deformity is often seen in Larsen syndrome. However, its progress in adults is not clear. The adjacent level compression in these patients adds to the difficulty regarding the level that needs to be operated. A 56-year-old male presented with neck pain and spastic quadriplegia. Radiology showed kyphotic deformity (sequelae of Larsen syndrome) with atlantoaxial dislocation. Cord compression was apparent at both levels but careful evaluation showed C1-2 level compression and some compression below the kyphotic deformity. The kyphotic spine was already fused and the canal diameter was adequate. The adjacent level C1-2 was fused and he improved dramatically. Correction of long-standing kyphotic deformity may not be necessary, as it unlikely to progress because of its tendency to fuse naturally. Rather, the adjacent levels are likely to compress the cord due to excessive stress. A proper clinical history and a thorough radiological examination help the surgeon to make an appropriate decision. </p>","PeriodicalId":520667,"journal":{"name":"Journal of craniovertebral junction & spine","volume":" ","pages":"109-10"},"PeriodicalIF":1.3000,"publicationDate":"2016-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/6e/ba/JCVJS-7-109.PMC4872559.pdf","citationCount":"8","resultStr":"{\"title\":\"Atlantoaxial dislocation adjacent to kyphotic deformity in a case of adult Larsen syndrome.\",\"authors\":\"Sushanta K Sahoo, Arsikere N Deepak, Pravin Salunke\",\"doi\":\"10.4103/0974-8237.181869\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Kyphotic deformity is often seen in Larsen syndrome. However, its progress in adults is not clear. The adjacent level compression in these patients adds to the difficulty regarding the level that needs to be operated. A 56-year-old male presented with neck pain and spastic quadriplegia. Radiology showed kyphotic deformity (sequelae of Larsen syndrome) with atlantoaxial dislocation. Cord compression was apparent at both levels but careful evaluation showed C1-2 level compression and some compression below the kyphotic deformity. The kyphotic spine was already fused and the canal diameter was adequate. The adjacent level C1-2 was fused and he improved dramatically. Correction of long-standing kyphotic deformity may not be necessary, as it unlikely to progress because of its tendency to fuse naturally. Rather, the adjacent levels are likely to compress the cord due to excessive stress. A proper clinical history and a thorough radiological examination help the surgeon to make an appropriate decision. </p>\",\"PeriodicalId\":520667,\"journal\":{\"name\":\"Journal of craniovertebral junction & spine\",\"volume\":\" \",\"pages\":\"109-10\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2016-04-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/6e/ba/JCVJS-7-109.PMC4872559.pdf\",\"citationCount\":\"8\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of craniovertebral junction & spine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4103/0974-8237.181869\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of craniovertebral junction & spine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/0974-8237.181869","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
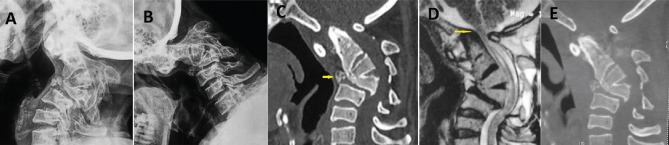
Atlantoaxial dislocation adjacent to kyphotic deformity in a case of adult Larsen syndrome.
Kyphotic deformity is often seen in Larsen syndrome. However, its progress in adults is not clear. The adjacent level compression in these patients adds to the difficulty regarding the level that needs to be operated. A 56-year-old male presented with neck pain and spastic quadriplegia. Radiology showed kyphotic deformity (sequelae of Larsen syndrome) with atlantoaxial dislocation. Cord compression was apparent at both levels but careful evaluation showed C1-2 level compression and some compression below the kyphotic deformity. The kyphotic spine was already fused and the canal diameter was adequate. The adjacent level C1-2 was fused and he improved dramatically. Correction of long-standing kyphotic deformity may not be necessary, as it unlikely to progress because of its tendency to fuse naturally. Rather, the adjacent levels are likely to compress the cord due to excessive stress. A proper clinical history and a thorough radiological examination help the surgeon to make an appropriate decision.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


