Lisa Rausch, Christian Koenecke, Hans-Friedrich Koch, Alexander Kaltenborn, Nikos Emmanouilidis, Lars Pape, Frank Lehner, Viktor Arelin, Ulrich Baumann, Harald Schrem
{"title":"配对分析:确定对肾脏或肝脏移植后发生 PTLD 有独立影响的因素。","authors":"Lisa Rausch, Christian Koenecke, Hans-Friedrich Koch, Alexander Kaltenborn, Nikos Emmanouilidis, Lars Pape, Frank Lehner, Viktor Arelin, Ulrich Baumann, Harald Schrem","doi":"10.1186/s13737-016-0036-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Post-transplant lymphoproliferative disorder (PTLD) adversely affects patients' long-term outcome.</p><p><strong>Methods: </strong>The paired t test and McNemar's test were applied in a retrospective 1:1 matched-pair analysis including 36 patients with PTLD and 36 patients without PTLD after kidney or liver transplantation. Matching criteria were age, gender, indication, type of transplantation, and duration of follow-up. All investigated PTLD specimen were histologically positive for EBV. Risk-adjusted multivariable regression analysis was used to identify independence of risk factors for PTLD detected in matched-pair analysis. The resultant prognostic model was assessed with ROC-curve analysis.</p><p><strong>Results: </strong>Patients suffering with PTLD had shorter mean survival (p = 0.004), more episodes of CMV infections or reactivations (p = 0.042), and fewer recipient HLA A2 haplotypes (p = 0.007), a tacrolimus-based immunosuppressive regimen (p = 0.052) and higher dosages of tacrolimus at hospital discharge (Tac dosage) (p = 0.052). Significant independent risk factors for PTLD were recipient HLA A2 (OR = 0.07, 95 % CI = 0.01-0.55, p = 0.011), higher Tac dosages (OR = 1.29, 95 % CI = 1.01-1.64, p = 0.040), and higher numbers of graft rejection episodes (OR = 0.38, 95 % CI = 0.17-0.87, p = 0.023). The following prognostic model for the prediction of PTLD demonstrated good model fit and a large area under the ROC curve (0.823): PTLD probability in % = Exp(y)/(1 + Exp(y)) with y = 0.671 - 1.096 × HLA A2-positive recipient + 0.151 × Tac dosage - 0.805 × number of graft rejection episodes.</p><p><strong>Conclusions: </strong>This study suggests prognostic relevance for recipient HLA A2, CMV, and EBV infections or reactivations and strong initial tacrolimus-based immunosuppression. Patients with risk factors may benefit from intensified screening for PTLD.</p>","PeriodicalId":89864,"journal":{"name":"Transplantation research","volume":"5 ","pages":"6"},"PeriodicalIF":0.0000,"publicationDate":"2016-08-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4970231/pdf/","citationCount":"0","resultStr":"{\"title\":\"Matched-pair analysis: identification of factors with independent influence on the development of PTLD after kidney or liver transplantation.\",\"authors\":\"Lisa Rausch, Christian Koenecke, Hans-Friedrich Koch, Alexander Kaltenborn, Nikos Emmanouilidis, Lars Pape, Frank Lehner, Viktor Arelin, Ulrich Baumann, Harald Schrem\",\"doi\":\"10.1186/s13737-016-0036-1\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Post-transplant lymphoproliferative disorder (PTLD) adversely affects patients' long-term outcome.</p><p><strong>Methods: </strong>The paired t test and McNemar's test were applied in a retrospective 1:1 matched-pair analysis including 36 patients with PTLD and 36 patients without PTLD after kidney or liver transplantation. Matching criteria were age, gender, indication, type of transplantation, and duration of follow-up. All investigated PTLD specimen were histologically positive for EBV. Risk-adjusted multivariable regression analysis was used to identify independence of risk factors for PTLD detected in matched-pair analysis. The resultant prognostic model was assessed with ROC-curve analysis.</p><p><strong>Results: </strong>Patients suffering with PTLD had shorter mean survival (p = 0.004), more episodes of CMV infections or reactivations (p = 0.042), and fewer recipient HLA A2 haplotypes (p = 0.007), a tacrolimus-based immunosuppressive regimen (p = 0.052) and higher dosages of tacrolimus at hospital discharge (Tac dosage) (p = 0.052). Significant independent risk factors for PTLD were recipient HLA A2 (OR = 0.07, 95 % CI = 0.01-0.55, p = 0.011), higher Tac dosages (OR = 1.29, 95 % CI = 1.01-1.64, p = 0.040), and higher numbers of graft rejection episodes (OR = 0.38, 95 % CI = 0.17-0.87, p = 0.023). The following prognostic model for the prediction of PTLD demonstrated good model fit and a large area under the ROC curve (0.823): PTLD probability in % = Exp(y)/(1 + Exp(y)) with y = 0.671 - 1.096 × HLA A2-positive recipient + 0.151 × Tac dosage - 0.805 × number of graft rejection episodes.</p><p><strong>Conclusions: </strong>This study suggests prognostic relevance for recipient HLA A2, CMV, and EBV infections or reactivations and strong initial tacrolimus-based immunosuppression. Patients with risk factors may benefit from intensified screening for PTLD.</p>\",\"PeriodicalId\":89864,\"journal\":{\"name\":\"Transplantation research\",\"volume\":\"5 \",\"pages\":\"6\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2016-08-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4970231/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Transplantation research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s13737-016-0036-1\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2016/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Transplantation research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13737-016-0036-1","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2016/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Methods: The paired t test and McNemar's test were applied in a retrospective 1:1 matched-pair analysis including 36 patients with PTLD and 36 patients without PTLD after kidney or liver transplantation. Matching criteria were age, gender, indication, type of transplantation, and duration of follow-up. All investigated PTLD specimen were histologically positive for EBV. Risk-adjusted multivariable regression analysis was used to identify independence of risk factors for PTLD detected in matched-pair analysis. The resultant prognostic model was assessed with ROC-curve analysis.
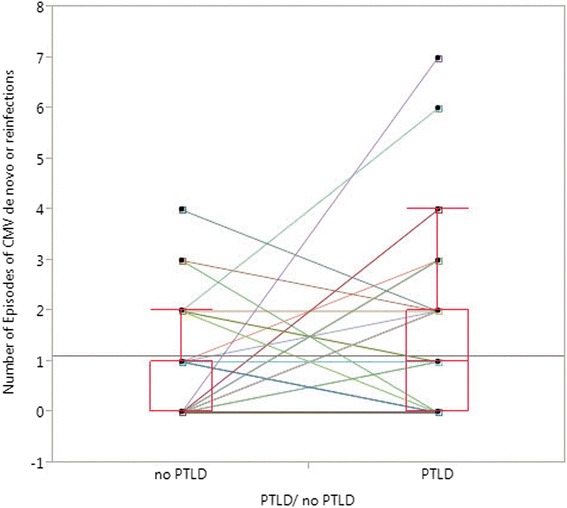
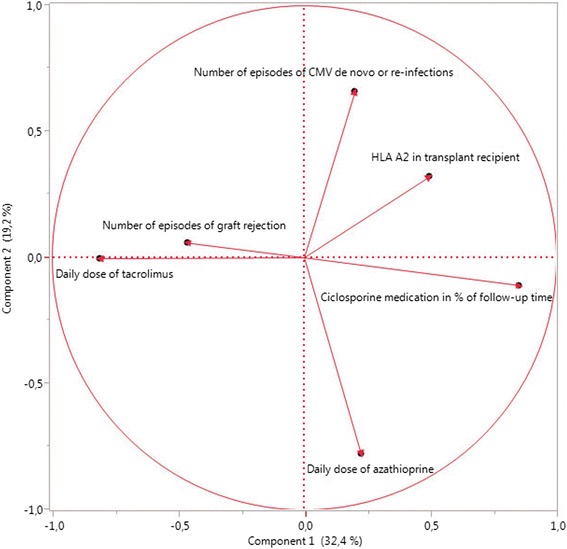
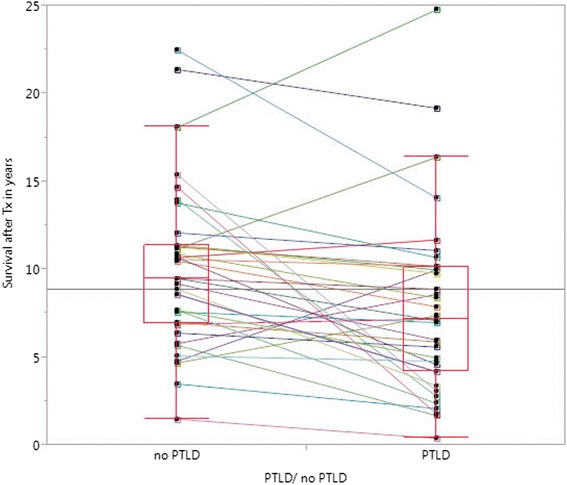
Results: Patients suffering with PTLD had shorter mean survival (p = 0.004), more episodes of CMV infections or reactivations (p = 0.042), and fewer recipient HLA A2 haplotypes (p = 0.007), a tacrolimus-based immunosuppressive regimen (p = 0.052) and higher dosages of tacrolimus at hospital discharge (Tac dosage) (p = 0.052). Significant independent risk factors for PTLD were recipient HLA A2 (OR = 0.07, 95 % CI = 0.01-0.55, p = 0.011), higher Tac dosages (OR = 1.29, 95 % CI = 1.01-1.64, p = 0.040), and higher numbers of graft rejection episodes (OR = 0.38, 95 % CI = 0.17-0.87, p = 0.023). The following prognostic model for the prediction of PTLD demonstrated good model fit and a large area under the ROC curve (0.823): PTLD probability in % = Exp(y)/(1 + Exp(y)) with y = 0.671 - 1.096 × HLA A2-positive recipient + 0.151 × Tac dosage - 0.805 × number of graft rejection episodes.
Conclusions: This study suggests prognostic relevance for recipient HLA A2, CMV, and EBV infections or reactivations and strong initial tacrolimus-based immunosuppression. Patients with risk factors may benefit from intensified screening for PTLD.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


