Hee Joon Kim, Choong Young Kim, Young Hoe Hur, Yang Seok Koh, Jung Chul Kim, Chol Kyoon Cho, Hyun Jong Kim
{"title":"肝切除术后残肝与总功能肝体积比和残肝与标准肝体积比作为术后肝功能预测指标的比较。","authors":"Hee Joon Kim, Choong Young Kim, Young Hoe Hur, Yang Seok Koh, Jung Chul Kim, Chol Kyoon Cho, Hyun Jong Kim","doi":"10.14701/kjhbps.2013.17.4.143","DOIUrl":null,"url":null,"abstract":"<p><strong>Backgrounds/aims: </strong>The future liver remnant (FLR) is usually calculated as a ratio of the remnant liver volume (RLV) to the total functional liver volume (RLV/TFLV). In liver transplantation, it is generally accepted that the ratio of the graft volume to standard liver volume (SLV) needs to be at least 30% to 40% to fit the hepatic metabolic demands of the recipient. The aim of this study was to compare RLV/TFLV versus RLV/SLV as a predictor of postoperative liver function and liver failure.</p><p><strong>Methods: </strong>CT volumetric measurements of RLV were obtained retrospectively in 74 patients who underwent right hemihepatectomy for a malignant tumor from January 2010 to May 2013. RLV and TFLV were obtained using CT volumetry, and SLV was calculated using Yu's formula: SLV (ml)=21.585×body weight (kg)(0.732)×height (cm)(0.225). The RLV/SLV ratio was compared with the RLV/TFLV as a predictor of postoperative hepatic function.</p><p><strong>Results: </strong>Postheptectomy liver failure (PHLF), morbidity, and serum total bilirubin level at postoperative day 5 (POD 5) were increased significantly in the group with the RLV/SLV ≤30% compared with the group with the RLV/SLV >30% (p=0.002, p=0.004, and p<0.001, respectively). But RLV/TFLV was not correlated with PHLF and morbidity (p=1.000 and 0.798, respectively). RLV/SLV showed a stronger correlation with serum total bilirubin level than RLV/TFLV (RLV/SLV vs. RLV/TFLV, R=0.706 vs. 0.499, R(2)=0.499 vs. 0.239).</p><p><strong>Conclusions: </strong>RLV/SLV was more specific than RLV/TFLV in predicting the postoperative course after right hemihepatectomy. To determine the safe limit of hepatic resection, a larger-scaled prospective study is needed.</p>","PeriodicalId":91136,"journal":{"name":"Korean journal of hepato-biliary-pancreatic surgery","volume":"17 4","pages":"143-51"},"PeriodicalIF":0.0000,"publicationDate":"2013-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.14701/kjhbps.2013.17.4.143","citationCount":"19","resultStr":"{\"title\":\"Comparison of remnant to total functional liver volume ratio and remnant to standard liver volume ratio as a predictor of postoperative liver function after liver resection.\",\"authors\":\"Hee Joon Kim, Choong Young Kim, Young Hoe Hur, Yang Seok Koh, Jung Chul Kim, Chol Kyoon Cho, Hyun Jong Kim\",\"doi\":\"10.14701/kjhbps.2013.17.4.143\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Backgrounds/aims: </strong>The future liver remnant (FLR) is usually calculated as a ratio of the remnant liver volume (RLV) to the total functional liver volume (RLV/TFLV). In liver transplantation, it is generally accepted that the ratio of the graft volume to standard liver volume (SLV) needs to be at least 30% to 40% to fit the hepatic metabolic demands of the recipient. The aim of this study was to compare RLV/TFLV versus RLV/SLV as a predictor of postoperative liver function and liver failure.</p><p><strong>Methods: </strong>CT volumetric measurements of RLV were obtained retrospectively in 74 patients who underwent right hemihepatectomy for a malignant tumor from January 2010 to May 2013. RLV and TFLV were obtained using CT volumetry, and SLV was calculated using Yu's formula: SLV (ml)=21.585×body weight (kg)(0.732)×height (cm)(0.225). The RLV/SLV ratio was compared with the RLV/TFLV as a predictor of postoperative hepatic function.</p><p><strong>Results: </strong>Postheptectomy liver failure (PHLF), morbidity, and serum total bilirubin level at postoperative day 5 (POD 5) were increased significantly in the group with the RLV/SLV ≤30% compared with the group with the RLV/SLV >30% (p=0.002, p=0.004, and p<0.001, respectively). But RLV/TFLV was not correlated with PHLF and morbidity (p=1.000 and 0.798, respectively). RLV/SLV showed a stronger correlation with serum total bilirubin level than RLV/TFLV (RLV/SLV vs. RLV/TFLV, R=0.706 vs. 0.499, R(2)=0.499 vs. 0.239).</p><p><strong>Conclusions: </strong>RLV/SLV was more specific than RLV/TFLV in predicting the postoperative course after right hemihepatectomy. To determine the safe limit of hepatic resection, a larger-scaled prospective study is needed.</p>\",\"PeriodicalId\":91136,\"journal\":{\"name\":\"Korean journal of hepato-biliary-pancreatic surgery\",\"volume\":\"17 4\",\"pages\":\"143-51\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2013-11-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.14701/kjhbps.2013.17.4.143\",\"citationCount\":\"19\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Korean journal of hepato-biliary-pancreatic surgery\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14701/kjhbps.2013.17.4.143\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2013/11/20 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Korean journal of hepato-biliary-pancreatic surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14701/kjhbps.2013.17.4.143","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2013/11/20 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Comparison of remnant to total functional liver volume ratio and remnant to standard liver volume ratio as a predictor of postoperative liver function after liver resection.
Backgrounds/aims: The future liver remnant (FLR) is usually calculated as a ratio of the remnant liver volume (RLV) to the total functional liver volume (RLV/TFLV). In liver transplantation, it is generally accepted that the ratio of the graft volume to standard liver volume (SLV) needs to be at least 30% to 40% to fit the hepatic metabolic demands of the recipient. The aim of this study was to compare RLV/TFLV versus RLV/SLV as a predictor of postoperative liver function and liver failure.
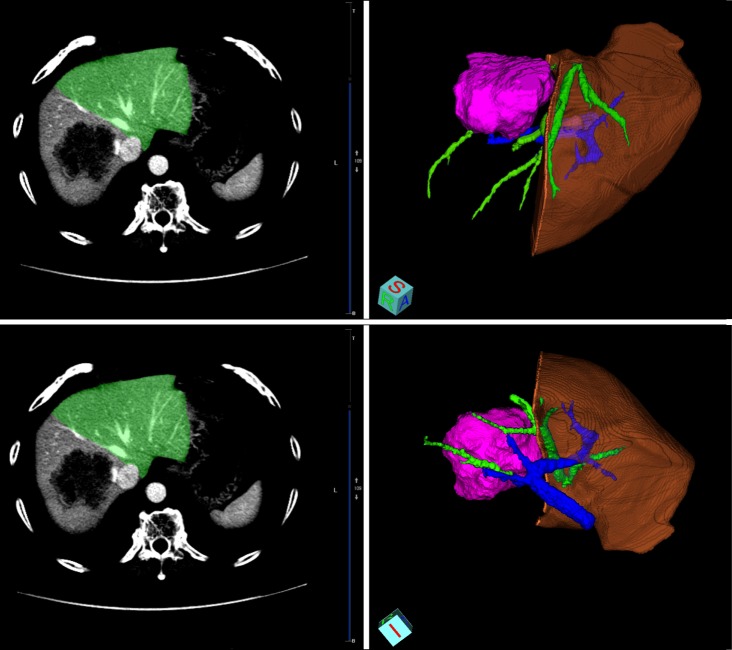
Methods: CT volumetric measurements of RLV were obtained retrospectively in 74 patients who underwent right hemihepatectomy for a malignant tumor from January 2010 to May 2013. RLV and TFLV were obtained using CT volumetry, and SLV was calculated using Yu's formula: SLV (ml)=21.585×body weight (kg)(0.732)×height (cm)(0.225). The RLV/SLV ratio was compared with the RLV/TFLV as a predictor of postoperative hepatic function.
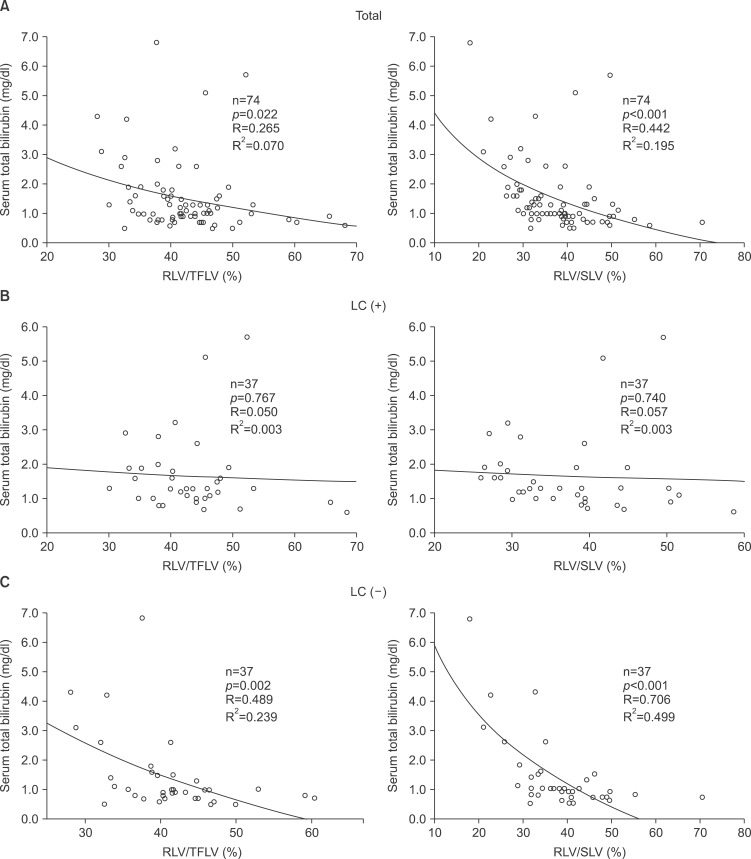
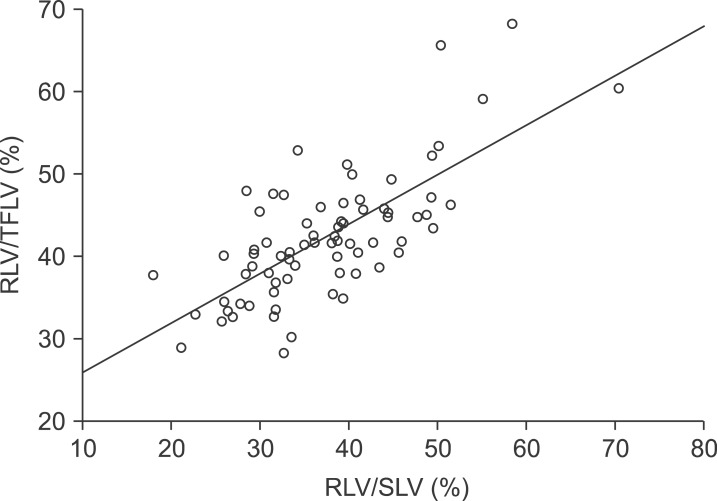
Results: Postheptectomy liver failure (PHLF), morbidity, and serum total bilirubin level at postoperative day 5 (POD 5) were increased significantly in the group with the RLV/SLV ≤30% compared with the group with the RLV/SLV >30% (p=0.002, p=0.004, and p<0.001, respectively). But RLV/TFLV was not correlated with PHLF and morbidity (p=1.000 and 0.798, respectively). RLV/SLV showed a stronger correlation with serum total bilirubin level than RLV/TFLV (RLV/SLV vs. RLV/TFLV, R=0.706 vs. 0.499, R(2)=0.499 vs. 0.239).
Conclusions: RLV/SLV was more specific than RLV/TFLV in predicting the postoperative course after right hemihepatectomy. To determine the safe limit of hepatic resection, a larger-scaled prospective study is needed.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


