Dalia Rotstein, Jacqueline M Solomon, Maria Pia Sormani, Xavier Montalban, Xiang Y Ye, Dina Dababneh, Alexandra Muccilli, Georges Saab, Prakesh Shah
{"title":"NEDA-4与多发性硬化症患者无长期残疾进展的相关性以及与NEDA-3的比较:一项系统综述和荟萃分析","authors":"Dalia Rotstein, Jacqueline M Solomon, Maria Pia Sormani, Xavier Montalban, Xiang Y Ye, Dina Dababneh, Alexandra Muccilli, Georges Saab, Prakesh Shah","doi":"10.1212/NXI.0000000000200032","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objectives: </strong>No evidence of disease activity (NEDA)-4 has been suggested as a treatment target for disease-modifying therapy (DMT) in relapsing-remitting multiple sclerosis (RRMS). However, the ability of NEDA-4 to discriminate long-term outcomes in MS and how its performance compares with NEDA-3 remain uncertain. We conducted a systematic review and meta-analysis to evaluate (1) the association between NEDA-4 and no long-term disability progression in MS and (2) the comparative performance of NEDA-3 and NEDA-4 in predicting no long-term disability progression.</p><p><strong>Methods: </strong>English-language abstracts and manuscripts were systematically searched in MEDLINE, Embase, and the Cochrane databases from January 2006 to November 2021 and reviewed independently by 2 investigators. We selected studies that assessed NEDA-4 at 1 or 2 years after DMT start and had at least 4 years of follow-up for determination of no confirmed disability progression. We conducted a meta-analysis using random-effects model to determine the pooled odds ratio (OR) for no disability progression with NEDA-4 vs EDA-4. For the comparative analysis, we selected studies that evaluated both NEDA-3 and NEDA-4 with at least 4 years of follow-up and examined the difference in the association of NEDA-3 and NEDA-4 with no disability progression.</p><p><strong>Results: </strong>Five studies of 1,000 patients (3 interferon beta and 2 fingolimod) met inclusion criteria for both objectives. The median duration of follow-up was 6 years (interquartile range: 4-6 years). The prevalence of NEDA-4 ranged from 4.2% to 13.9% on interferon beta therapy and 24.9% to 25.1% on fingolimod therapy. The pooled OR for no long-term confirmed disability progression with NEDA-4 vs EDA-4 was 2.14 (95% confidence interval: 1.36-3.37; I<sup>2</sup> = 0). We did not observe any significant difference between NEDA-4 and NEDA-3 in the comparative analyses.</p><p><strong>Discussion: </strong>In patients with RRMS, NEDA-4 at 1-2 years was associated with 2 times higher odds of no long-term disability progression, at 6 years compared with EDA-4, but offered no advantage over NEDA-3.</p>","PeriodicalId":520720,"journal":{"name":"Neurology(R) neuroimmunology & neuroinflammation","volume":" ","pages":""},"PeriodicalIF":7.5000,"publicationDate":"2022-10-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/e3/ac/NXI-2022-200038.PMC9558627.pdf","citationCount":"5","resultStr":"{\"title\":\"Association of NEDA-4 With No Long-term Disability Progression in Multiple Sclerosis and Comparison With NEDA-3: A Systematic Review and Meta-analysis.\",\"authors\":\"Dalia Rotstein, Jacqueline M Solomon, Maria Pia Sormani, Xavier Montalban, Xiang Y Ye, Dina Dababneh, Alexandra Muccilli, Georges Saab, Prakesh Shah\",\"doi\":\"10.1212/NXI.0000000000200032\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background and objectives: </strong>No evidence of disease activity (NEDA)-4 has been suggested as a treatment target for disease-modifying therapy (DMT) in relapsing-remitting multiple sclerosis (RRMS). However, the ability of NEDA-4 to discriminate long-term outcomes in MS and how its performance compares with NEDA-3 remain uncertain. We conducted a systematic review and meta-analysis to evaluate (1) the association between NEDA-4 and no long-term disability progression in MS and (2) the comparative performance of NEDA-3 and NEDA-4 in predicting no long-term disability progression.</p><p><strong>Methods: </strong>English-language abstracts and manuscripts were systematically searched in MEDLINE, Embase, and the Cochrane databases from January 2006 to November 2021 and reviewed independently by 2 investigators. We selected studies that assessed NEDA-4 at 1 or 2 years after DMT start and had at least 4 years of follow-up for determination of no confirmed disability progression. We conducted a meta-analysis using random-effects model to determine the pooled odds ratio (OR) for no disability progression with NEDA-4 vs EDA-4. For the comparative analysis, we selected studies that evaluated both NEDA-3 and NEDA-4 with at least 4 years of follow-up and examined the difference in the association of NEDA-3 and NEDA-4 with no disability progression.</p><p><strong>Results: </strong>Five studies of 1,000 patients (3 interferon beta and 2 fingolimod) met inclusion criteria for both objectives. The median duration of follow-up was 6 years (interquartile range: 4-6 years). The prevalence of NEDA-4 ranged from 4.2% to 13.9% on interferon beta therapy and 24.9% to 25.1% on fingolimod therapy. The pooled OR for no long-term confirmed disability progression with NEDA-4 vs EDA-4 was 2.14 (95% confidence interval: 1.36-3.37; I<sup>2</sup> = 0). We did not observe any significant difference between NEDA-4 and NEDA-3 in the comparative analyses.</p><p><strong>Discussion: </strong>In patients with RRMS, NEDA-4 at 1-2 years was associated with 2 times higher odds of no long-term disability progression, at 6 years compared with EDA-4, but offered no advantage over NEDA-3.</p>\",\"PeriodicalId\":520720,\"journal\":{\"name\":\"Neurology(R) neuroimmunology & neuroinflammation\",\"volume\":\" \",\"pages\":\"\"},\"PeriodicalIF\":7.5000,\"publicationDate\":\"2022-10-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/e3/ac/NXI-2022-200038.PMC9558627.pdf\",\"citationCount\":\"5\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neurology(R) neuroimmunology & neuroinflammation\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1212/NXI.0000000000200032\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/11/1 0:00:00\",\"PubModel\":\"Print\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurology(R) neuroimmunology & neuroinflammation","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1212/NXI.0000000000200032","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/11/1 0:00:00","PubModel":"Print","JCR":"","JCRName":"","Score":null,"Total":0}
Association of NEDA-4 With No Long-term Disability Progression in Multiple Sclerosis and Comparison With NEDA-3: A Systematic Review and Meta-analysis.
Background and objectives: No evidence of disease activity (NEDA)-4 has been suggested as a treatment target for disease-modifying therapy (DMT) in relapsing-remitting multiple sclerosis (RRMS). However, the ability of NEDA-4 to discriminate long-term outcomes in MS and how its performance compares with NEDA-3 remain uncertain. We conducted a systematic review and meta-analysis to evaluate (1) the association between NEDA-4 and no long-term disability progression in MS and (2) the comparative performance of NEDA-3 and NEDA-4 in predicting no long-term disability progression.
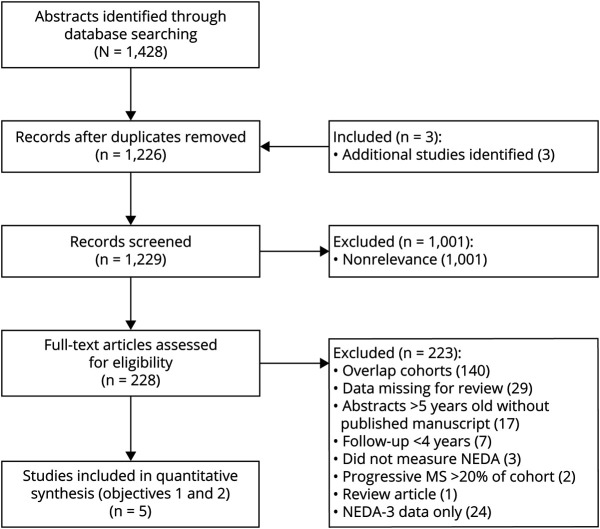
Methods: English-language abstracts and manuscripts were systematically searched in MEDLINE, Embase, and the Cochrane databases from January 2006 to November 2021 and reviewed independently by 2 investigators. We selected studies that assessed NEDA-4 at 1 or 2 years after DMT start and had at least 4 years of follow-up for determination of no confirmed disability progression. We conducted a meta-analysis using random-effects model to determine the pooled odds ratio (OR) for no disability progression with NEDA-4 vs EDA-4. For the comparative analysis, we selected studies that evaluated both NEDA-3 and NEDA-4 with at least 4 years of follow-up and examined the difference in the association of NEDA-3 and NEDA-4 with no disability progression.
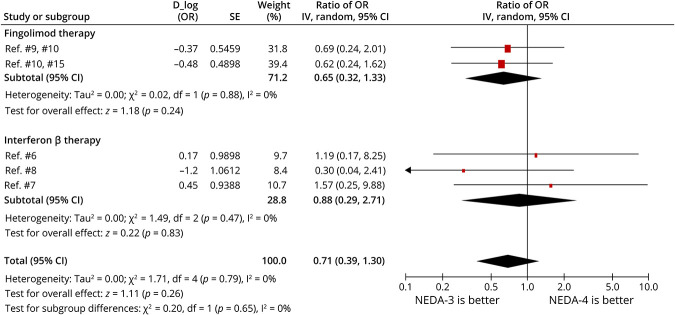
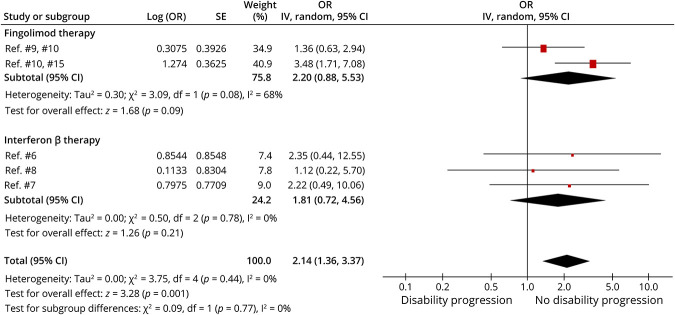
Results: Five studies of 1,000 patients (3 interferon beta and 2 fingolimod) met inclusion criteria for both objectives. The median duration of follow-up was 6 years (interquartile range: 4-6 years). The prevalence of NEDA-4 ranged from 4.2% to 13.9% on interferon beta therapy and 24.9% to 25.1% on fingolimod therapy. The pooled OR for no long-term confirmed disability progression with NEDA-4 vs EDA-4 was 2.14 (95% confidence interval: 1.36-3.37; I2 = 0). We did not observe any significant difference between NEDA-4 and NEDA-3 in the comparative analyses.
Discussion: In patients with RRMS, NEDA-4 at 1-2 years was associated with 2 times higher odds of no long-term disability progression, at 6 years compared with EDA-4, but offered no advantage over NEDA-3.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


