{"title":"1例结核分枝杆菌感染患者口服不能耐受,静脉注射含泰地唑胺治疗成功。","authors":"Haruka Karaushi, Masafumi Seki, Yutaka Miyawaki, Noriyuki Watanabe, Fumitaka Kamoshita, Kotaro Mitsutake","doi":"10.12659/AJCR.937485","DOIUrl":null,"url":null,"abstract":"<p><p>BACKGROUND Mycobacterium tuberculosis (M. tuberculosis) is usually treated by oral antimycobacterial agents, including rifampicin, ethambutol, and pyrazinamide, but the treatment regimen with intravenous and/or intramuscular antimycobacterial agents for patients who cannot take medications orally remains unclear. CASE REPORT A 77-year-old man with chronic renal failure had an esophageal-skin fistula after he had surgeries for removal of esophageal and gastric cancers and reconstruction using jejunum, and he showed a cavity, tree-in-bud formation, and pleural effusions in his left upper lung fields on his chest X-ray after treatment of cellulitis and bacteremia/candidemia by meropenem, teicoplanin, and micafungin. M. tuberculosis was isolated from his sputum and exudate fluid from the reconstructed esophageal-skin fistula. Although he could not take antimycobacterial agents orally, treatment was started with intravenous agents combining levofloxacin (LVFX) every other day, isoniazid (INH), and linezolid (LZD). However, his platelets were decreased 21 days after treatment started, and it was thought to be an adverse effect of LZD and/or INH. After changing LZD to tedizolid (TZD), in addition to changing from INH to intramuscular streptomycin twice per week, his platelet counts increased. Intravenous TZD could be continued, and it maintained his condition without exacerbations of thrombocytopenia and renal failure. The M. tuberculosis disappeared, and the abnormal chest X-ray shadows were improved 2 months after the start of treatment. CONCLUSIONS Administration of intravenous TZD, in addition to intravenous LVFX and intramuscular SM in combination, might be a candidate regimen for M. tuberculosis patients who cannot take oral medications.</p>","PeriodicalId":205256,"journal":{"name":"The American Journal of Case Reports","volume":" ","pages":"e937485"},"PeriodicalIF":0.0000,"publicationDate":"2022-10-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/c0/cf/amjcaserep-23-e937485.PMC9562597.pdf","citationCount":"0","resultStr":"{\"title\":\"A Mycobacterium tuberculosis-Infected Patient Who Could Not Tolerate Oral Intake Successfully Treated Using an Intravenous Tedizolid-Containing Regimen.\",\"authors\":\"Haruka Karaushi, Masafumi Seki, Yutaka Miyawaki, Noriyuki Watanabe, Fumitaka Kamoshita, Kotaro Mitsutake\",\"doi\":\"10.12659/AJCR.937485\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>BACKGROUND Mycobacterium tuberculosis (M. tuberculosis) is usually treated by oral antimycobacterial agents, including rifampicin, ethambutol, and pyrazinamide, but the treatment regimen with intravenous and/or intramuscular antimycobacterial agents for patients who cannot take medications orally remains unclear. CASE REPORT A 77-year-old man with chronic renal failure had an esophageal-skin fistula after he had surgeries for removal of esophageal and gastric cancers and reconstruction using jejunum, and he showed a cavity, tree-in-bud formation, and pleural effusions in his left upper lung fields on his chest X-ray after treatment of cellulitis and bacteremia/candidemia by meropenem, teicoplanin, and micafungin. M. tuberculosis was isolated from his sputum and exudate fluid from the reconstructed esophageal-skin fistula. Although he could not take antimycobacterial agents orally, treatment was started with intravenous agents combining levofloxacin (LVFX) every other day, isoniazid (INH), and linezolid (LZD). However, his platelets were decreased 21 days after treatment started, and it was thought to be an adverse effect of LZD and/or INH. After changing LZD to tedizolid (TZD), in addition to changing from INH to intramuscular streptomycin twice per week, his platelet counts increased. Intravenous TZD could be continued, and it maintained his condition without exacerbations of thrombocytopenia and renal failure. The M. tuberculosis disappeared, and the abnormal chest X-ray shadows were improved 2 months after the start of treatment. CONCLUSIONS Administration of intravenous TZD, in addition to intravenous LVFX and intramuscular SM in combination, might be a candidate regimen for M. tuberculosis patients who cannot take oral medications.</p>\",\"PeriodicalId\":205256,\"journal\":{\"name\":\"The American Journal of Case Reports\",\"volume\":\" \",\"pages\":\"e937485\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-10-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/c0/cf/amjcaserep-23-e937485.PMC9562597.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"The American Journal of Case Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.12659/AJCR.937485\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"The American Journal of Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.12659/AJCR.937485","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
A Mycobacterium tuberculosis-Infected Patient Who Could Not Tolerate Oral Intake Successfully Treated Using an Intravenous Tedizolid-Containing Regimen.
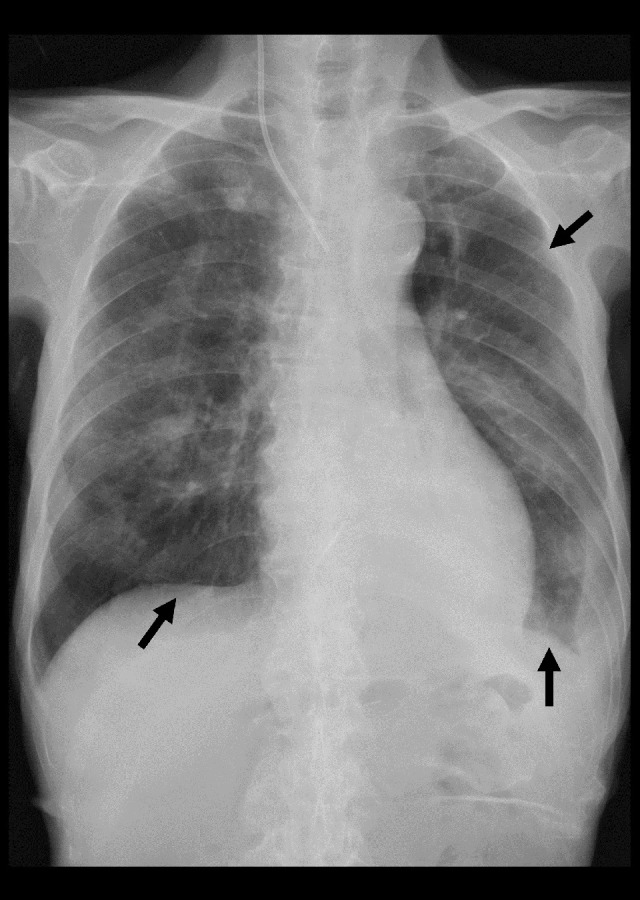
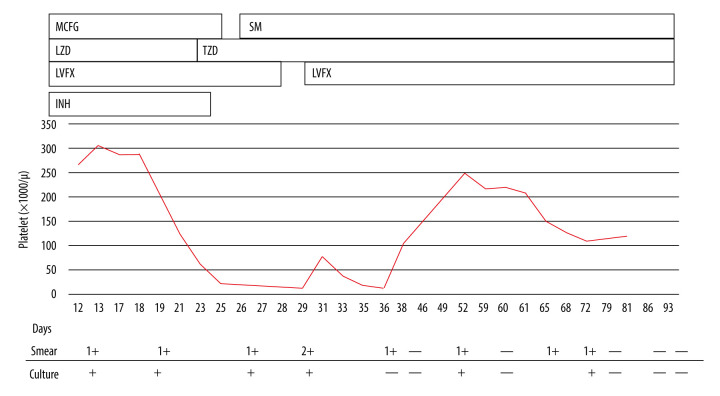
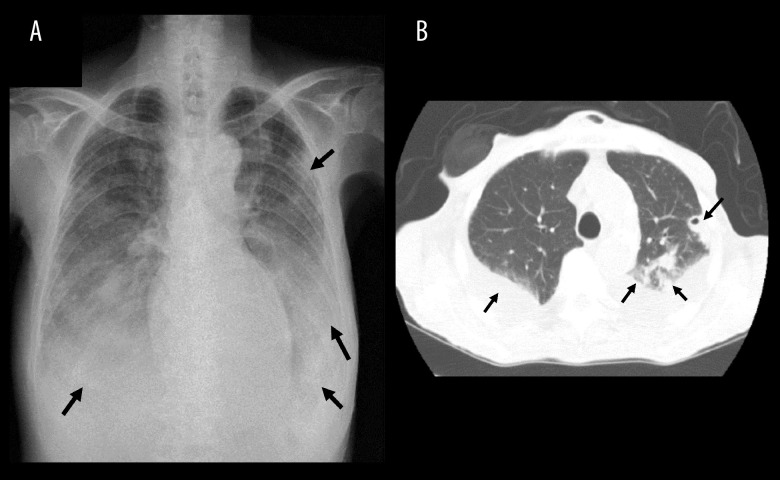
BACKGROUND Mycobacterium tuberculosis (M. tuberculosis) is usually treated by oral antimycobacterial agents, including rifampicin, ethambutol, and pyrazinamide, but the treatment regimen with intravenous and/or intramuscular antimycobacterial agents for patients who cannot take medications orally remains unclear. CASE REPORT A 77-year-old man with chronic renal failure had an esophageal-skin fistula after he had surgeries for removal of esophageal and gastric cancers and reconstruction using jejunum, and he showed a cavity, tree-in-bud formation, and pleural effusions in his left upper lung fields on his chest X-ray after treatment of cellulitis and bacteremia/candidemia by meropenem, teicoplanin, and micafungin. M. tuberculosis was isolated from his sputum and exudate fluid from the reconstructed esophageal-skin fistula. Although he could not take antimycobacterial agents orally, treatment was started with intravenous agents combining levofloxacin (LVFX) every other day, isoniazid (INH), and linezolid (LZD). However, his platelets were decreased 21 days after treatment started, and it was thought to be an adverse effect of LZD and/or INH. After changing LZD to tedizolid (TZD), in addition to changing from INH to intramuscular streptomycin twice per week, his platelet counts increased. Intravenous TZD could be continued, and it maintained his condition without exacerbations of thrombocytopenia and renal failure. The M. tuberculosis disappeared, and the abnormal chest X-ray shadows were improved 2 months after the start of treatment. CONCLUSIONS Administration of intravenous TZD, in addition to intravenous LVFX and intramuscular SM in combination, might be a candidate regimen for M. tuberculosis patients who cannot take oral medications.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


