{"title":"急性偏头痛发作静脉注射甲氧氯普胺减轻疼痛和不良反应:随机对照试验的系统回顾和荟萃分析。","authors":"Nat Ungrungseesopon, Wachira Wongtanasarasin","doi":"10.5662/wjm.v12.i4.319","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Metoclopramide may be used to treat people suffering from acute migraine. However, no comprehensive investigation on this issue has been recorded. This review will provide more solid evidence for the use of metoclopramide in treating acute migraine.</p><p><strong>Aim: </strong>To compare the efficacy of intravenous metoclopramide with other therapies in migraine attack treatment in an emergency department (ED).</p><p><strong>Methods: </strong>We included randomized controlled trials of participants older than 18 years with acute migraine headaches, which included at least one arm that received intravenous (IV) metoclopramide at the ED. A literature search of PubMed, Web of Science, Cochrane Collaboration, and Reference Citation Analysis on December 31, 2021 retrieved other drugs or placebo-controlled studies without language limitation. The risk of bias was assessed using the Cochrane risk of bias tool. The primary endpoint was pain reduction at 60 min or closest to 1 h after treatment, as measured by the pain scale. Secondary endpoints included adverse effects or reactions resulting from metoclopramide or comparisons.</p><p><strong>Results: </strong>Fourteen trials with a total of 1661 individuals were eligible for review. The risk of bias ranged from low to intermediate. IV metoclopramide administration was not associated with higher pain reduction at 1 h (Standard mean difference [SMD] = -0.03, 95% confidence interval [CI]: -0.33-0.28, <i>P</i> = 0.87). However, metoclopramide was associated with better pain reduction than placebo (SMD = 1.04, 95%CI: 0.50-1.58, <i>P</i> = 0.0002). In addition, side effects were not significantly different between IV metoclopramide and other drugs or placebo (odds ratio [OR] = 0.76, 95%CI: 0.48-1.19, <i>P</i> = 0.09 and OR = 0.92, 95%CI: 0.31-2.74, <i>P</i> = 0.54, respectively).</p><p><strong>Conclusion: </strong>Metoclopramide is more effective than placebo in treating migraine in the ED. Despite the observed tendency of decreased side effects, its effectiveness compared to other regimens is poorly understood. More research on this area is needed to treat migraine in acute care settings effectively.</p>","PeriodicalId":23729,"journal":{"name":"World journal of methodology","volume":"12 4","pages":"319-330"},"PeriodicalIF":0.0000,"publicationDate":"2022-07-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/b6/9e/WJM-12-319.PMC9350726.pdf","citationCount":"1","resultStr":"{\"title\":\"Pain reduction and adverse effects of intravenous metoclopramide for acute migraine attack: A systematic review and meta-analysis of randomized-controlled trials.\",\"authors\":\"Nat Ungrungseesopon, Wachira Wongtanasarasin\",\"doi\":\"10.5662/wjm.v12.i4.319\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Metoclopramide may be used to treat people suffering from acute migraine. However, no comprehensive investigation on this issue has been recorded. This review will provide more solid evidence for the use of metoclopramide in treating acute migraine.</p><p><strong>Aim: </strong>To compare the efficacy of intravenous metoclopramide with other therapies in migraine attack treatment in an emergency department (ED).</p><p><strong>Methods: </strong>We included randomized controlled trials of participants older than 18 years with acute migraine headaches, which included at least one arm that received intravenous (IV) metoclopramide at the ED. A literature search of PubMed, Web of Science, Cochrane Collaboration, and Reference Citation Analysis on December 31, 2021 retrieved other drugs or placebo-controlled studies without language limitation. The risk of bias was assessed using the Cochrane risk of bias tool. The primary endpoint was pain reduction at 60 min or closest to 1 h after treatment, as measured by the pain scale. Secondary endpoints included adverse effects or reactions resulting from metoclopramide or comparisons.</p><p><strong>Results: </strong>Fourteen trials with a total of 1661 individuals were eligible for review. The risk of bias ranged from low to intermediate. IV metoclopramide administration was not associated with higher pain reduction at 1 h (Standard mean difference [SMD] = -0.03, 95% confidence interval [CI]: -0.33-0.28, <i>P</i> = 0.87). However, metoclopramide was associated with better pain reduction than placebo (SMD = 1.04, 95%CI: 0.50-1.58, <i>P</i> = 0.0002). In addition, side effects were not significantly different between IV metoclopramide and other drugs or placebo (odds ratio [OR] = 0.76, 95%CI: 0.48-1.19, <i>P</i> = 0.09 and OR = 0.92, 95%CI: 0.31-2.74, <i>P</i> = 0.54, respectively).</p><p><strong>Conclusion: </strong>Metoclopramide is more effective than placebo in treating migraine in the ED. Despite the observed tendency of decreased side effects, its effectiveness compared to other regimens is poorly understood. More research on this area is needed to treat migraine in acute care settings effectively.</p>\",\"PeriodicalId\":23729,\"journal\":{\"name\":\"World journal of methodology\",\"volume\":\"12 4\",\"pages\":\"319-330\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-07-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/b6/9e/WJM-12-319.PMC9350726.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"World journal of methodology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5662/wjm.v12.i4.319\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"World journal of methodology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5662/wjm.v12.i4.319","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
摘要
背景:甲氧氯普胺可用于治疗急性偏头痛患者。然而,没有关于这一问题的全面调查记录。本综述将为甲氧氯普胺治疗急性偏头痛提供更有力的证据。目的:比较静脉注射甲氧氯普胺与其他治疗方法在急诊科治疗偏头痛发作中的疗效。方法:我们纳入了18岁以上急性偏头痛患者的随机对照试验,其中至少有一组患者在急症室接受静脉注射(IV)甲氯普胺。PubMed、Web of Science、Cochrane Collaboration和Reference Citation Analysis于2021年12月31日检索了其他药物或无语言限制的安慰剂对照研究。使用Cochrane偏倚风险工具评估偏倚风险。主要终点是治疗后60分钟或接近1小时的疼痛减轻,根据疼痛量表测量。次要终点包括甲氧氯普胺或比较物引起的不良反应或反应。结果:14项试验共1661名受试者符合审查条件。偏倚风险从低到中等。静脉注射甲氧氯普胺与1小时疼痛减轻程度无关(标准均差[SMD] = -0.03, 95%可信区间[CI]: -0.33-0.28, P = 0.87)。然而,与安慰剂相比,甲氧氯普胺能更好地减轻疼痛(SMD = 1.04, 95%CI: 0.50-1.58, P = 0.0002)。此外,静脉注射甲氧氯普胺与其他药物或安慰剂的副作用无显著差异(优势比[or] = 0.76, 95%CI: 0.48 ~ 1.19, P = 0.09; or = 0.92, 95%CI: 0.31 ~ 2.74, P = 0.54)。结论:甲氧氯普胺治疗ED偏头痛比安慰剂更有效。尽管观察到副作用减少的趋势,但与其他方案相比,其有效性尚不清楚。在这方面需要更多的研究,以有效地治疗急性护理环境中的偏头痛。
Pain reduction and adverse effects of intravenous metoclopramide for acute migraine attack: A systematic review and meta-analysis of randomized-controlled trials.
Background: Metoclopramide may be used to treat people suffering from acute migraine. However, no comprehensive investigation on this issue has been recorded. This review will provide more solid evidence for the use of metoclopramide in treating acute migraine.
Aim: To compare the efficacy of intravenous metoclopramide with other therapies in migraine attack treatment in an emergency department (ED).
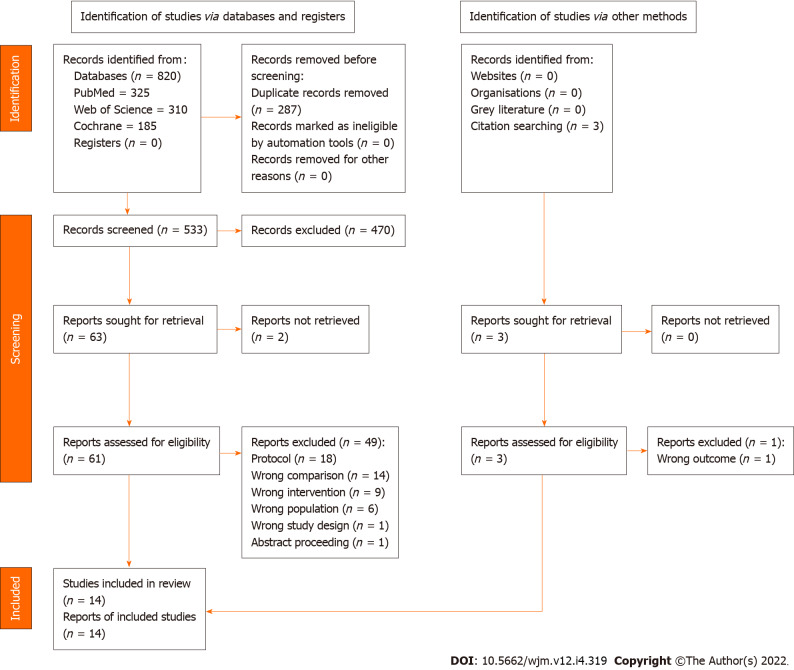
Methods: We included randomized controlled trials of participants older than 18 years with acute migraine headaches, which included at least one arm that received intravenous (IV) metoclopramide at the ED. A literature search of PubMed, Web of Science, Cochrane Collaboration, and Reference Citation Analysis on December 31, 2021 retrieved other drugs or placebo-controlled studies without language limitation. The risk of bias was assessed using the Cochrane risk of bias tool. The primary endpoint was pain reduction at 60 min or closest to 1 h after treatment, as measured by the pain scale. Secondary endpoints included adverse effects or reactions resulting from metoclopramide or comparisons.
Results: Fourteen trials with a total of 1661 individuals were eligible for review. The risk of bias ranged from low to intermediate. IV metoclopramide administration was not associated with higher pain reduction at 1 h (Standard mean difference [SMD] = -0.03, 95% confidence interval [CI]: -0.33-0.28, P = 0.87). However, metoclopramide was associated with better pain reduction than placebo (SMD = 1.04, 95%CI: 0.50-1.58, P = 0.0002). In addition, side effects were not significantly different between IV metoclopramide and other drugs or placebo (odds ratio [OR] = 0.76, 95%CI: 0.48-1.19, P = 0.09 and OR = 0.92, 95%CI: 0.31-2.74, P = 0.54, respectively).
Conclusion: Metoclopramide is more effective than placebo in treating migraine in the ED. Despite the observed tendency of decreased side effects, its effectiveness compared to other regimens is poorly understood. More research on this area is needed to treat migraine in acute care settings effectively.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


