Alberto Federico García, Fernando Rodríguez, Álvaro Sánchez, Isabella Caicedo-Holguín, Carlos Gallego-Navarro, María Paula Naranjo, Yaset Caicedo, Daniela Burbano, Diana Felisa Currea-Perdomo, Carlos A Ordoñez, Juan Carlos Puyana
{"title":"膈肌创伤后脓胸的危险因素。","authors":"Alberto Federico García, Fernando Rodríguez, Álvaro Sánchez, Isabella Caicedo-Holguín, Carlos Gallego-Navarro, María Paula Naranjo, Yaset Caicedo, Daniela Burbano, Diana Felisa Currea-Perdomo, Carlos A Ordoñez, Juan Carlos Puyana","doi":"10.1186/s13017-022-00453-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Penetrating diaphragmatic injuries are associated with a high incidence of posttraumatic empyema. We analyzed the contribution of trauma severity, specific organ injury, contamination severity, and surgical management to the risk of posttraumatic empyema in patients who underwent surgical repair of diaphragmatic injuries at a level 1 trauma center.</p><p><strong>Methods: </strong>This is a retrospective review of the patients who survived more than 48 h. Univariate OR calculations were performed to identify potential risk factors. Multiple logistic regression was used to calculate adjusted ORs and identify independent risk factors.</p><p><strong>Results: </strong>We included 192 patients treated from 2011 to 2020. There were 169 (88.0) males. The mean interquartile range, (IQR) of age, was 27 (22-35) years. Gunshot injuries occurred in 155 subjects (80.7%). Mean (IQR) NISS and ATI were 29 (18-44) and 17 (10-27), respectively. Thoracic AIS was > 3 in 38 patients (19.8%). Hollow viscus was injured in 105 cases (54.7%): stomach in 65 (33.9%), colon in 52 (27.1%), small bowel in 42 (21.9%), and duodenum in 10 (5.2%). Visible contamination was found in 76 patients (39.6%). Potential thoracic contamination was managed with a chest tube in 128 cases (66.7%), with transdiaphragmatic pleural lavage in 42 (21.9%), and with video-assisted thoracoscopy surgery or thoracotomy in 22 (11.5%). Empyema occurred in 11 patients (5.7%). Multiple logistic regression identified thoracic AIS > 3 (OR 6.4, 95% CI 1.77-23. 43), and visible contamination (OR 5.13, 95% IC 1.26-20.90) as independent risk factors. The individual organ injured, or the method used to manage the thoracic contamination did not affect the risk of posttraumatic empyema.</p><p><strong>Conclusion: </strong>The severity of the thoracic injury and the presence of visible abdominal contamination were identified as independent risk factors for empyema after penetrating diaphragmatic trauma.</p>","PeriodicalId":290899,"journal":{"name":"World Journal of Emergency Surgery : WJES","volume":" ","pages":"47"},"PeriodicalIF":0.0000,"publicationDate":"2022-09-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9472425/pdf/","citationCount":"0","resultStr":"{\"title\":\"Risk factors for posttraumatic empyema in diaphragmatic injuries.\",\"authors\":\"Alberto Federico García, Fernando Rodríguez, Álvaro Sánchez, Isabella Caicedo-Holguín, Carlos Gallego-Navarro, María Paula Naranjo, Yaset Caicedo, Daniela Burbano, Diana Felisa Currea-Perdomo, Carlos A Ordoñez, Juan Carlos Puyana\",\"doi\":\"10.1186/s13017-022-00453-9\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Penetrating diaphragmatic injuries are associated with a high incidence of posttraumatic empyema. We analyzed the contribution of trauma severity, specific organ injury, contamination severity, and surgical management to the risk of posttraumatic empyema in patients who underwent surgical repair of diaphragmatic injuries at a level 1 trauma center.</p><p><strong>Methods: </strong>This is a retrospective review of the patients who survived more than 48 h. Univariate OR calculations were performed to identify potential risk factors. Multiple logistic regression was used to calculate adjusted ORs and identify independent risk factors.</p><p><strong>Results: </strong>We included 192 patients treated from 2011 to 2020. There were 169 (88.0) males. The mean interquartile range, (IQR) of age, was 27 (22-35) years. Gunshot injuries occurred in 155 subjects (80.7%). Mean (IQR) NISS and ATI were 29 (18-44) and 17 (10-27), respectively. Thoracic AIS was > 3 in 38 patients (19.8%). Hollow viscus was injured in 105 cases (54.7%): stomach in 65 (33.9%), colon in 52 (27.1%), small bowel in 42 (21.9%), and duodenum in 10 (5.2%). Visible contamination was found in 76 patients (39.6%). Potential thoracic contamination was managed with a chest tube in 128 cases (66.7%), with transdiaphragmatic pleural lavage in 42 (21.9%), and with video-assisted thoracoscopy surgery or thoracotomy in 22 (11.5%). Empyema occurred in 11 patients (5.7%). Multiple logistic regression identified thoracic AIS > 3 (OR 6.4, 95% CI 1.77-23. 43), and visible contamination (OR 5.13, 95% IC 1.26-20.90) as independent risk factors. The individual organ injured, or the method used to manage the thoracic contamination did not affect the risk of posttraumatic empyema.</p><p><strong>Conclusion: </strong>The severity of the thoracic injury and the presence of visible abdominal contamination were identified as independent risk factors for empyema after penetrating diaphragmatic trauma.</p>\",\"PeriodicalId\":290899,\"journal\":{\"name\":\"World Journal of Emergency Surgery : WJES\",\"volume\":\" \",\"pages\":\"47\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-09-13\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9472425/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"World Journal of Emergency Surgery : WJES\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s13017-022-00453-9\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Emergency Surgery : WJES","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13017-022-00453-9","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景:穿透性横膈膜损伤与创伤后脓胸的高发有关。我们分析了创伤严重程度、特定器官损伤、污染严重程度和手术处理对在一级创伤中心接受膈肌损伤手术修复的患者创伤后脓胸风险的影响。方法:对存活超过48小时的患者进行回顾性分析。进行单因素OR计算以确定潜在的危险因素。采用多元logistic回归计算调整后的or并识别独立危险因素。结果:我们纳入了2011年至2020年治疗的192例患者。男性169人(88.0人)。年龄的平均四分位数范围(IQR)为27(22-35)岁。枪击伤155例(80.7%)。NISS和ATI的平均(IQR)分别为29(18-44)和17(10-27)。38例(19.8%)胸椎AIS > 3。其中,胃损伤65例(33.9%),结肠损伤52例(27.1%),小肠损伤42例(21.9%),十二指肠损伤10例(5.2%)。可见污染76例(39.6%)。128例(66.7%)采用胸管,42例(21.9%)采用经膈胸腔灌洗,22例(11.5%)采用电视胸腔镜手术或开胸。11例(5.7%)发生脓胸。多元logistic回归鉴定胸部AIS > 3 (OR 6.4, 95% CI 1.77-23)。43)和可见污染(OR 5.13, 95% IC 1.26-20.90)为独立危险因素。个体器官损伤或处理胸廓污染的方法不影响创伤后脓胸的风险。结论:胸椎损伤的严重程度和可见的腹部污染是横膈膜穿透伤后发生脓胸的独立危险因素。
Risk factors for posttraumatic empyema in diaphragmatic injuries.
Background: Penetrating diaphragmatic injuries are associated with a high incidence of posttraumatic empyema. We analyzed the contribution of trauma severity, specific organ injury, contamination severity, and surgical management to the risk of posttraumatic empyema in patients who underwent surgical repair of diaphragmatic injuries at a level 1 trauma center.
Methods: This is a retrospective review of the patients who survived more than 48 h. Univariate OR calculations were performed to identify potential risk factors. Multiple logistic regression was used to calculate adjusted ORs and identify independent risk factors.
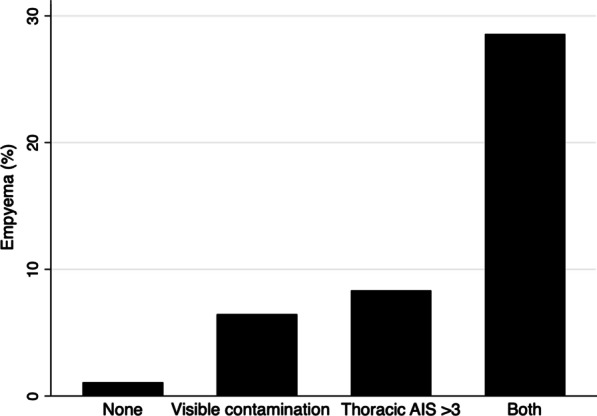
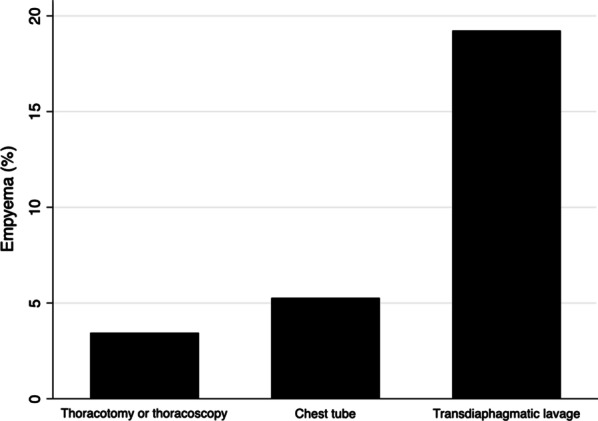
Results: We included 192 patients treated from 2011 to 2020. There were 169 (88.0) males. The mean interquartile range, (IQR) of age, was 27 (22-35) years. Gunshot injuries occurred in 155 subjects (80.7%). Mean (IQR) NISS and ATI were 29 (18-44) and 17 (10-27), respectively. Thoracic AIS was > 3 in 38 patients (19.8%). Hollow viscus was injured in 105 cases (54.7%): stomach in 65 (33.9%), colon in 52 (27.1%), small bowel in 42 (21.9%), and duodenum in 10 (5.2%). Visible contamination was found in 76 patients (39.6%). Potential thoracic contamination was managed with a chest tube in 128 cases (66.7%), with transdiaphragmatic pleural lavage in 42 (21.9%), and with video-assisted thoracoscopy surgery or thoracotomy in 22 (11.5%). Empyema occurred in 11 patients (5.7%). Multiple logistic regression identified thoracic AIS > 3 (OR 6.4, 95% CI 1.77-23. 43), and visible contamination (OR 5.13, 95% IC 1.26-20.90) as independent risk factors. The individual organ injured, or the method used to manage the thoracic contamination did not affect the risk of posttraumatic empyema.
Conclusion: The severity of the thoracic injury and the presence of visible abdominal contamination were identified as independent risk factors for empyema after penetrating diaphragmatic trauma.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


