Andrea Péter, Ágnes Balogh, Zoltán Csanádi, Katalin Dankó, Zoltan Griger
{"title":"多相多发性肌炎/皮肌炎的亚临床收缩和舒张心肌功能障碍:一项为期2年的纵向研究。","authors":"Andrea Péter, Ágnes Balogh, Zoltán Csanádi, Katalin Dankó, Zoltan Griger","doi":"10.1186/s13075-022-02906-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Cardiac involvement in patients with idiopathic inflammatory myopathies (IIM) is associated with increased morbidity and mortality risk; however, little is known about the progression of cardiac dysfunction and long-term data are scarce. In the present work, we intended to prospectively study echocardiographic parameters in patients with IIM for 2 years.</p><p><strong>Methods: </strong>Twenty-eight IIM patients (41.9±1.6 years) without cardiovascular symptoms were enrolled. Patients with monophasic/polyphasic disease patterns were studied separately and compared to age-matched healthy individuals. Conventional echocardiographic and tissue Doppler imaging (TDI) parameters of systolic [LV: ejection fraction (EF), mitral annulus systolic movement (MAPSE), lateral s') and diastolic left (mitral inflow velocities, lateral anulus velocities: e', a', E/e') and right ventricular function (fractional area change: FAC, tricuspid annulus plane systolic excursion: TAPSE) were measured at the time of the diagnosis and 2 years later.</p><p><strong>Results: </strong>Subclinical LV systolic dysfunction is characterized by reduced lateral s' (10.4 vs. 6.4 cm/s, p<0.05), EF (62.6±0.6%, vs. 51.7±0.7%) and MAPSE (18.5±0.6 vs. 14.5±0.6 mm) could be observed in IIM patients with polyphasic disease course 2 years after diagnosis compared to controls. Furthermore, diastolic LV function showed a marked deterioration to grade I diastolic dysfunction at 2 years in the polyphasic group (lateral e': 12.9 ±0.6, vs. 7.4±0.3 cm/s; lateral a': 10.7±0.3, vs. 17.3±0.8 cm/s; p<0.05) supported by larger left atrium (32.1±0.6 vs. 37.8±0.6 mm; p<0.05]. TDI measurements confirmed subclinical RV systolic dysfunction in polyphasic patients 2 years after diagnosis (FAC: 45.6±1.8%, vs. 32.7±1.4%; TAPSE: 22.7±0.5, vs. 18.1±0.3 mm; p<0.05). Similar, but not significant tendencies could be detected in patients with monophasic disease patterns. Polyphasic patients showed significantly (p<0.05) worse results compared to monophasic patients regarding EF (51.7±0.7% vs. 58.1±0.6%), lateral s' (6.4±0.4 cm/sec vs. 8.6±0.4 cm/s,), left atrium (37.8±0.6 mm vs. 33.3±0.8 mm), FAC (32.7±1.4% vs. 41.0±1.6%) and TAPSE (18.1±0.3 mm vs. 21.3±0.7 mm).</p><p><strong>Conclusions: </strong>Significant subclinical cardiac dysfunction could be detected in IIM patients with polyphasic disease course 2 years after diagnosis, which identifies them as a high-risk population. TDI is a useful method to detect echocardiographic abnormalities in IIM complementing conventional echocardiography and can recognize the high cardiac risk.</p>","PeriodicalId":51225,"journal":{"name":"Arthritis Research & Therapy","volume":"24 1","pages":"219"},"PeriodicalIF":4.6000,"publicationDate":"2022-09-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9463723/pdf/","citationCount":"1","resultStr":"{\"title\":\"Subclinical systolic and diastolic myocardial dysfunction in polyphasic polymyositis/dermatomyositis: a 2-year longitudinal study.\",\"authors\":\"Andrea Péter, Ágnes Balogh, Zoltán Csanádi, Katalin Dankó, Zoltan Griger\",\"doi\":\"10.1186/s13075-022-02906-7\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Cardiac involvement in patients with idiopathic inflammatory myopathies (IIM) is associated with increased morbidity and mortality risk; however, little is known about the progression of cardiac dysfunction and long-term data are scarce. In the present work, we intended to prospectively study echocardiographic parameters in patients with IIM for 2 years.</p><p><strong>Methods: </strong>Twenty-eight IIM patients (41.9±1.6 years) without cardiovascular symptoms were enrolled. Patients with monophasic/polyphasic disease patterns were studied separately and compared to age-matched healthy individuals. Conventional echocardiographic and tissue Doppler imaging (TDI) parameters of systolic [LV: ejection fraction (EF), mitral annulus systolic movement (MAPSE), lateral s') and diastolic left (mitral inflow velocities, lateral anulus velocities: e', a', E/e') and right ventricular function (fractional area change: FAC, tricuspid annulus plane systolic excursion: TAPSE) were measured at the time of the diagnosis and 2 years later.</p><p><strong>Results: </strong>Subclinical LV systolic dysfunction is characterized by reduced lateral s' (10.4 vs. 6.4 cm/s, p<0.05), EF (62.6±0.6%, vs. 51.7±0.7%) and MAPSE (18.5±0.6 vs. 14.5±0.6 mm) could be observed in IIM patients with polyphasic disease course 2 years after diagnosis compared to controls. Furthermore, diastolic LV function showed a marked deterioration to grade I diastolic dysfunction at 2 years in the polyphasic group (lateral e': 12.9 ±0.6, vs. 7.4±0.3 cm/s; lateral a': 10.7±0.3, vs. 17.3±0.8 cm/s; p<0.05) supported by larger left atrium (32.1±0.6 vs. 37.8±0.6 mm; p<0.05]. TDI measurements confirmed subclinical RV systolic dysfunction in polyphasic patients 2 years after diagnosis (FAC: 45.6±1.8%, vs. 32.7±1.4%; TAPSE: 22.7±0.5, vs. 18.1±0.3 mm; p<0.05). Similar, but not significant tendencies could be detected in patients with monophasic disease patterns. Polyphasic patients showed significantly (p<0.05) worse results compared to monophasic patients regarding EF (51.7±0.7% vs. 58.1±0.6%), lateral s' (6.4±0.4 cm/sec vs. 8.6±0.4 cm/s,), left atrium (37.8±0.6 mm vs. 33.3±0.8 mm), FAC (32.7±1.4% vs. 41.0±1.6%) and TAPSE (18.1±0.3 mm vs. 21.3±0.7 mm).</p><p><strong>Conclusions: </strong>Significant subclinical cardiac dysfunction could be detected in IIM patients with polyphasic disease course 2 years after diagnosis, which identifies them as a high-risk population. TDI is a useful method to detect echocardiographic abnormalities in IIM complementing conventional echocardiography and can recognize the high cardiac risk.</p>\",\"PeriodicalId\":51225,\"journal\":{\"name\":\"Arthritis Research & Therapy\",\"volume\":\"24 1\",\"pages\":\"219\"},\"PeriodicalIF\":4.6000,\"publicationDate\":\"2022-09-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9463723/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Arthritis Research & Therapy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s13075-022-02906-7\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"RHEUMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Arthritis Research & Therapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13075-022-02906-7","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
引用次数: 1
摘要
背景:特发性炎症性肌病(IIM)患者的心脏受累与发病率和死亡率增加相关;然而,对心功能障碍的进展知之甚少,长期数据也很缺乏。在目前的工作中,我们打算前瞻性地研究2年IIM患者的超声心动图参数。方法:纳入28例无心血管症状的IIM患者(41.9±1.6岁)。患有单相/多相疾病模式的患者被单独研究,并与年龄匹配的健康个体进行比较。常规超声心动图和组织多普勒成像(TDI)参数[左室:射血分数(EF),二尖瓣环收缩运动(MAPSE),外侧s']和舒张左室(二尖瓣血流速度,外侧环速度:e', a', e /e')和右室功能(分数面积变化:FAC,三尖瓣环平面收缩偏移:TAPSE)在诊断时和2年后测量。结果:亚临床左室收缩功能障碍的特征是侧侧s′减小(10.4 vs. 6.4 cm/s)。结论:IIM多相病程2年后可检测到显著的亚临床心功能障碍,为高危人群。TDI是检测IIM超声心动图异常的一种有效方法,是对常规超声心动图的补充,可以识别心脏高危人群。
Subclinical systolic and diastolic myocardial dysfunction in polyphasic polymyositis/dermatomyositis: a 2-year longitudinal study.
Background: Cardiac involvement in patients with idiopathic inflammatory myopathies (IIM) is associated with increased morbidity and mortality risk; however, little is known about the progression of cardiac dysfunction and long-term data are scarce. In the present work, we intended to prospectively study echocardiographic parameters in patients with IIM for 2 years.
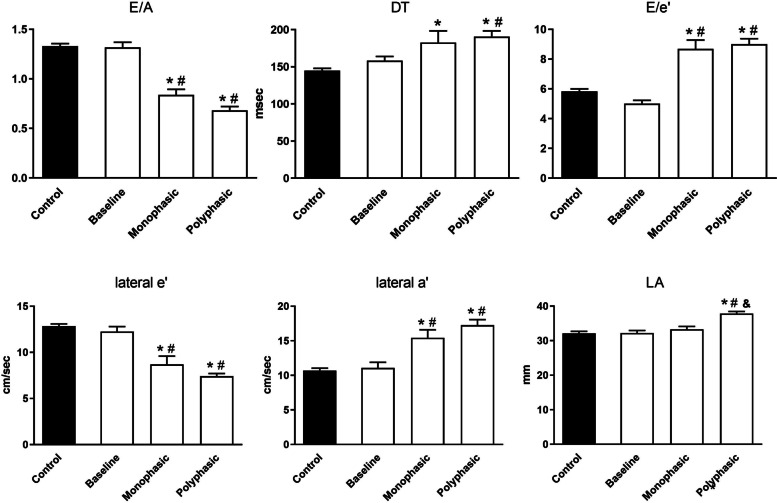
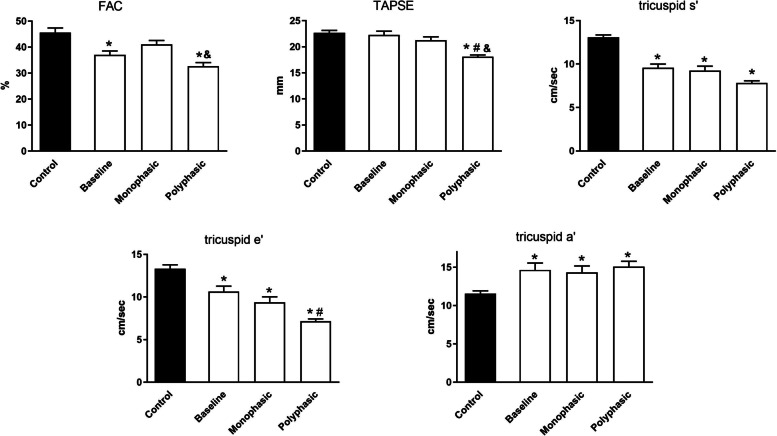
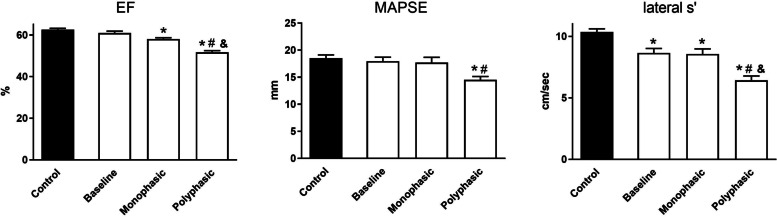
Methods: Twenty-eight IIM patients (41.9±1.6 years) without cardiovascular symptoms were enrolled. Patients with monophasic/polyphasic disease patterns were studied separately and compared to age-matched healthy individuals. Conventional echocardiographic and tissue Doppler imaging (TDI) parameters of systolic [LV: ejection fraction (EF), mitral annulus systolic movement (MAPSE), lateral s') and diastolic left (mitral inflow velocities, lateral anulus velocities: e', a', E/e') and right ventricular function (fractional area change: FAC, tricuspid annulus plane systolic excursion: TAPSE) were measured at the time of the diagnosis and 2 years later.
Results: Subclinical LV systolic dysfunction is characterized by reduced lateral s' (10.4 vs. 6.4 cm/s, p<0.05), EF (62.6±0.6%, vs. 51.7±0.7%) and MAPSE (18.5±0.6 vs. 14.5±0.6 mm) could be observed in IIM patients with polyphasic disease course 2 years after diagnosis compared to controls. Furthermore, diastolic LV function showed a marked deterioration to grade I diastolic dysfunction at 2 years in the polyphasic group (lateral e': 12.9 ±0.6, vs. 7.4±0.3 cm/s; lateral a': 10.7±0.3, vs. 17.3±0.8 cm/s; p<0.05) supported by larger left atrium (32.1±0.6 vs. 37.8±0.6 mm; p<0.05]. TDI measurements confirmed subclinical RV systolic dysfunction in polyphasic patients 2 years after diagnosis (FAC: 45.6±1.8%, vs. 32.7±1.4%; TAPSE: 22.7±0.5, vs. 18.1±0.3 mm; p<0.05). Similar, but not significant tendencies could be detected in patients with monophasic disease patterns. Polyphasic patients showed significantly (p<0.05) worse results compared to monophasic patients regarding EF (51.7±0.7% vs. 58.1±0.6%), lateral s' (6.4±0.4 cm/sec vs. 8.6±0.4 cm/s,), left atrium (37.8±0.6 mm vs. 33.3±0.8 mm), FAC (32.7±1.4% vs. 41.0±1.6%) and TAPSE (18.1±0.3 mm vs. 21.3±0.7 mm).
Conclusions: Significant subclinical cardiac dysfunction could be detected in IIM patients with polyphasic disease course 2 years after diagnosis, which identifies them as a high-risk population. TDI is a useful method to detect echocardiographic abnormalities in IIM complementing conventional echocardiography and can recognize the high cardiac risk.
期刊介绍:
Established in 1999, Arthritis Research and Therapy is an international, open access, peer-reviewed journal, publishing original articles in the area of musculoskeletal research and therapy as well as, reviews, commentaries and reports.
A major focus of the journal is on the immunologic processes leading to inflammation, damage and repair as they relate to autoimmune rheumatic and musculoskeletal conditions, and which inform the translation of this knowledge into advances in clinical care.
Original basic, translational and clinical research is considered for publication along with results of early and late phase therapeutic trials, especially as they pertain to the underpinning science that informs clinical observations in interventional studies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


