Wendell Zhang, Lee Yung Wong, Jasmine Liu, Soham Sarkar
{"title":"紧急情况下的不良反应监测(MONKEY)——对住院请求被拒绝的急诊患者处理结果的审计。","authors":"Wendell Zhang, Lee Yung Wong, Jasmine Liu, Soham Sarkar","doi":"10.2147/OAEM.S376419","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Emergency Department (ED) clinicians commonly experience difficulties in referring patients to inpatient teams for hospital admission. There is limited literature reporting on patient outcomes following these complicated referrals, where ED requests for inpatient admission are rejected - which study investigators termed a \"knockback\".</p><p><strong>Purpose: </strong>To identify disposition outcomes and referral accuracy in ED patients whose admission referral was initially rejected. Secondary objectives were to identify additional patient, clinician and systemic factors associated with knockbacks.</p><p><strong>Selection and methodology: </strong>Emergency clinicians prospectively nominated a convenience sample of patients identified as having knockbacks over two time periods (Jan-Feb 2020 and Aug 2020 to Jan 2021) at a tertiary Australian ED. Data were analyzed with a mixed-methods approach and subsequent descriptive and thematic analyses were performed.</p><p><strong>Results: </strong>A total of 109 patients were identified as knockbacks. The referrals were warranted, with 89.0% of cases (n = 97) ultimately requiring a hospital admission. In 60.6% (n = 66) of the admissions, patients were admitted under the inpatient team initially referred to by the ED, suggesting referrals were generally accurate. The number of in-hospital units involved in the admission process and ED length of stay were positively correlated (0.409, p < 0.001). Patient factors associated with knockbacks include pre-existing chronic medical conditions and presenting acutely unwell. Analysis of clinicians' perspectives yielded recurring themes of disagreements over admission destination and diagnostic uncertainty.</p><p><strong>Conclusion: </strong>In this patient sample, emergency referrals for admission were mostly warranted and accurate. Knockbacks increase ED length of stay and may adversely affect patient care. Further focused discussion and clearer referral guidelines between ED clinicians and their inpatient colleagues are required.</p>","PeriodicalId":503614,"journal":{"name":"Open Access Emergency Medicine : OAEM","volume":" ","pages":"481-490"},"PeriodicalIF":0.0000,"publicationDate":"2022-09-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/9b/a6/oaem-14-481.PMC9448349.pdf","citationCount":"1","resultStr":"{\"title\":\"MONitoring Knockbacks in EmergencY (MONKEY) - An Audit of Disposition Outcomes in Emergency Patients with Rejected Admission Requests.\",\"authors\":\"Wendell Zhang, Lee Yung Wong, Jasmine Liu, Soham Sarkar\",\"doi\":\"10.2147/OAEM.S376419\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Emergency Department (ED) clinicians commonly experience difficulties in referring patients to inpatient teams for hospital admission. There is limited literature reporting on patient outcomes following these complicated referrals, where ED requests for inpatient admission are rejected - which study investigators termed a \\\"knockback\\\".</p><p><strong>Purpose: </strong>To identify disposition outcomes and referral accuracy in ED patients whose admission referral was initially rejected. Secondary objectives were to identify additional patient, clinician and systemic factors associated with knockbacks.</p><p><strong>Selection and methodology: </strong>Emergency clinicians prospectively nominated a convenience sample of patients identified as having knockbacks over two time periods (Jan-Feb 2020 and Aug 2020 to Jan 2021) at a tertiary Australian ED. Data were analyzed with a mixed-methods approach and subsequent descriptive and thematic analyses were performed.</p><p><strong>Results: </strong>A total of 109 patients were identified as knockbacks. The referrals were warranted, with 89.0% of cases (n = 97) ultimately requiring a hospital admission. In 60.6% (n = 66) of the admissions, patients were admitted under the inpatient team initially referred to by the ED, suggesting referrals were generally accurate. The number of in-hospital units involved in the admission process and ED length of stay were positively correlated (0.409, p < 0.001). Patient factors associated with knockbacks include pre-existing chronic medical conditions and presenting acutely unwell. Analysis of clinicians' perspectives yielded recurring themes of disagreements over admission destination and diagnostic uncertainty.</p><p><strong>Conclusion: </strong>In this patient sample, emergency referrals for admission were mostly warranted and accurate. Knockbacks increase ED length of stay and may adversely affect patient care. Further focused discussion and clearer referral guidelines between ED clinicians and their inpatient colleagues are required.</p>\",\"PeriodicalId\":503614,\"journal\":{\"name\":\"Open Access Emergency Medicine : OAEM\",\"volume\":\" \",\"pages\":\"481-490\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-09-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/9b/a6/oaem-14-481.PMC9448349.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Open Access Emergency Medicine : OAEM\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/OAEM.S376419\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open Access Emergency Medicine : OAEM","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/OAEM.S376419","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
MONitoring Knockbacks in EmergencY (MONKEY) - An Audit of Disposition Outcomes in Emergency Patients with Rejected Admission Requests.
Background: Emergency Department (ED) clinicians commonly experience difficulties in referring patients to inpatient teams for hospital admission. There is limited literature reporting on patient outcomes following these complicated referrals, where ED requests for inpatient admission are rejected - which study investigators termed a "knockback".
Purpose: To identify disposition outcomes and referral accuracy in ED patients whose admission referral was initially rejected. Secondary objectives were to identify additional patient, clinician and systemic factors associated with knockbacks.
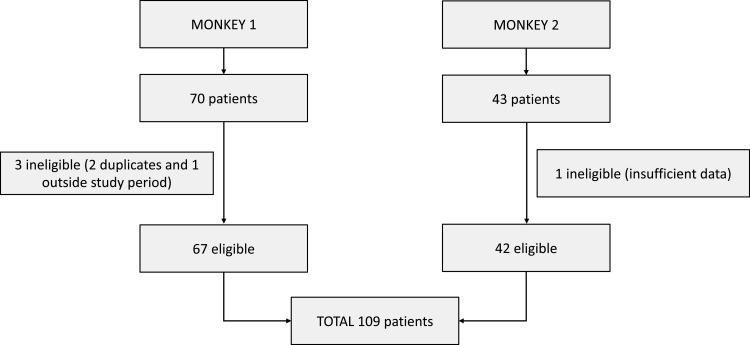
Selection and methodology: Emergency clinicians prospectively nominated a convenience sample of patients identified as having knockbacks over two time periods (Jan-Feb 2020 and Aug 2020 to Jan 2021) at a tertiary Australian ED. Data were analyzed with a mixed-methods approach and subsequent descriptive and thematic analyses were performed.
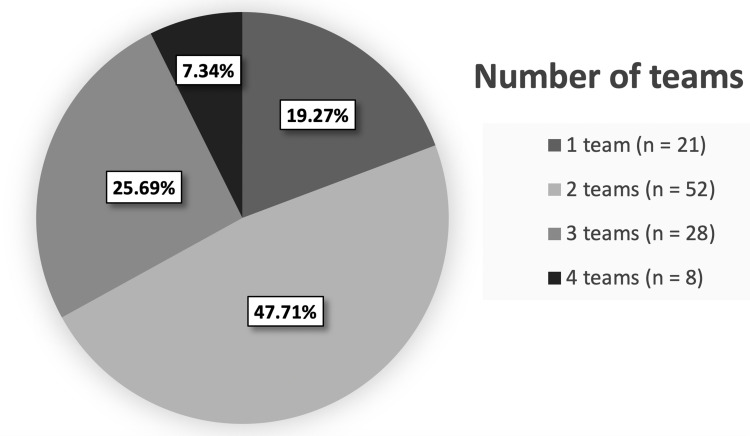
Results: A total of 109 patients were identified as knockbacks. The referrals were warranted, with 89.0% of cases (n = 97) ultimately requiring a hospital admission. In 60.6% (n = 66) of the admissions, patients were admitted under the inpatient team initially referred to by the ED, suggesting referrals were generally accurate. The number of in-hospital units involved in the admission process and ED length of stay were positively correlated (0.409, p < 0.001). Patient factors associated with knockbacks include pre-existing chronic medical conditions and presenting acutely unwell. Analysis of clinicians' perspectives yielded recurring themes of disagreements over admission destination and diagnostic uncertainty.
Conclusion: In this patient sample, emergency referrals for admission were mostly warranted and accurate. Knockbacks increase ED length of stay and may adversely affect patient care. Further focused discussion and clearer referral guidelines between ED clinicians and their inpatient colleagues are required.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


