Ghulam Saydain, Aamir Awan, Palaniappan Manickam, Paul Kleinow, Safwan Badr
{"title":"肺动脉高压是重症监护病房死亡的独立危险因素:血流动力学因素与死亡率的相关性。","authors":"Ghulam Saydain, Aamir Awan, Palaniappan Manickam, Paul Kleinow, Safwan Badr","doi":"10.4137/CCRPM.S22199","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Critically ill patients with pulmonary hypertension (PH) pose additional challenges due to the existence of right ventricular (RV) dysfunction. The purpose of this study was to assess the impact of hemodynamic factors on the outcome.</p><p><strong>Methods: </strong>We reviewed the records of patients with a diagnosis of PH admitted to the intensive care unit. In addition to evaluating traditional hemodynamic parameters, we defined severe PH as right atrial pressure >20 mmHg, mean pulmonary artery pressure >55 mmHg, or cardiac index (CI) <2 L/min/m(2). We also defined the RV functional index (RFI) as pulmonary artery systolic pressure (PASP) adjusted for CI as PASP/CI; increasing values reflect RV dysfunction.</p><p><strong>Results: </strong>Fifty-three patients (mean age 60 years, 72% women, 79% Blacks), were included in the study. Severe PH was present in 68% of patients who had higher Sequential Organ Failure Assessment (SOFA) score (6.8 ± 3.3 vs 3.8 ± 1.6; P = 0.001) and overall in-hospital mortality (36% vs 6%; P = 0.02) compared to nonsevere patients, although Acute Physiology and Chronic Health Evaluation (APACHE) II scores (19.9 ± 7.5 vs 18.5 ± 6.04; P = 0.52) were similar and sepsis was more frequent among nonsevere PH patients (31 vs 64%; P = 0.02). Severe PH (P = 0.04), lower mean arterial pressure (P = 0.04), and CI (P = 0.01); need for invasive ventilation (P = 0.02) and vasopressors (P = 0.03); and higher SOFA (P = 0.001), APACHE II (P = 0.03), pulmonary vascular resistance index (PVRI) (P = 0.01), and RFI (P = 0.004) were associated with increased mortality. In a multivariate model, SOFA [OR = 1.45, 95% confidence interval (C.I.) = 1.09-1.93; P = 0.01], PVRI (OR = 1.12, 95% C.I. = 1.02-1.24; P = 0.02), and increasing RFI (OR = 1.06, 95% C.I. = 1.01-1.11; P = 0.01) were independently associated with mortality.</p><p><strong>Conclusion: </strong>PH is an independent risk factor for mortality in critically ill patients. Composite factors rather than individual hemodynamic parameters are better predictors of outcome. Monitoring of RV function using composite hemodynamic factors resulting in specific interventions is likely to improve survival and needs to be studied further.</p>","PeriodicalId":44269,"journal":{"name":"Clinical Medicine Insights-Circulatory Respiratory and Pulmonary Medicine","volume":"9 ","pages":"27-33"},"PeriodicalIF":0.9000,"publicationDate":"2015-06-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.4137/CCRPM.S22199","citationCount":"21","resultStr":"{\"title\":\"Pulmonary Hypertension an Independent Risk Factor for Death in Intensive Care Unit: Correlation of Hemodynamic Factors with Mortality.\",\"authors\":\"Ghulam Saydain, Aamir Awan, Palaniappan Manickam, Paul Kleinow, Safwan Badr\",\"doi\":\"10.4137/CCRPM.S22199\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>Critically ill patients with pulmonary hypertension (PH) pose additional challenges due to the existence of right ventricular (RV) dysfunction. The purpose of this study was to assess the impact of hemodynamic factors on the outcome.</p><p><strong>Methods: </strong>We reviewed the records of patients with a diagnosis of PH admitted to the intensive care unit. In addition to evaluating traditional hemodynamic parameters, we defined severe PH as right atrial pressure >20 mmHg, mean pulmonary artery pressure >55 mmHg, or cardiac index (CI) <2 L/min/m(2). We also defined the RV functional index (RFI) as pulmonary artery systolic pressure (PASP) adjusted for CI as PASP/CI; increasing values reflect RV dysfunction.</p><p><strong>Results: </strong>Fifty-three patients (mean age 60 years, 72% women, 79% Blacks), were included in the study. Severe PH was present in 68% of patients who had higher Sequential Organ Failure Assessment (SOFA) score (6.8 ± 3.3 vs 3.8 ± 1.6; P = 0.001) and overall in-hospital mortality (36% vs 6%; P = 0.02) compared to nonsevere patients, although Acute Physiology and Chronic Health Evaluation (APACHE) II scores (19.9 ± 7.5 vs 18.5 ± 6.04; P = 0.52) were similar and sepsis was more frequent among nonsevere PH patients (31 vs 64%; P = 0.02). Severe PH (P = 0.04), lower mean arterial pressure (P = 0.04), and CI (P = 0.01); need for invasive ventilation (P = 0.02) and vasopressors (P = 0.03); and higher SOFA (P = 0.001), APACHE II (P = 0.03), pulmonary vascular resistance index (PVRI) (P = 0.01), and RFI (P = 0.004) were associated with increased mortality. In a multivariate model, SOFA [OR = 1.45, 95% confidence interval (C.I.) = 1.09-1.93; P = 0.01], PVRI (OR = 1.12, 95% C.I. = 1.02-1.24; P = 0.02), and increasing RFI (OR = 1.06, 95% C.I. = 1.01-1.11; P = 0.01) were independently associated with mortality.</p><p><strong>Conclusion: </strong>PH is an independent risk factor for mortality in critically ill patients. Composite factors rather than individual hemodynamic parameters are better predictors of outcome. Monitoring of RV function using composite hemodynamic factors resulting in specific interventions is likely to improve survival and needs to be studied further.</p>\",\"PeriodicalId\":44269,\"journal\":{\"name\":\"Clinical Medicine Insights-Circulatory Respiratory and Pulmonary Medicine\",\"volume\":\"9 \",\"pages\":\"27-33\"},\"PeriodicalIF\":0.9000,\"publicationDate\":\"2015-06-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.4137/CCRPM.S22199\",\"citationCount\":\"21\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Medicine Insights-Circulatory Respiratory and Pulmonary Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4137/CCRPM.S22199\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2015/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine Insights-Circulatory Respiratory and Pulmonary Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4137/CCRPM.S22199","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2015/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
Pulmonary Hypertension an Independent Risk Factor for Death in Intensive Care Unit: Correlation of Hemodynamic Factors with Mortality.
Objective: Critically ill patients with pulmonary hypertension (PH) pose additional challenges due to the existence of right ventricular (RV) dysfunction. The purpose of this study was to assess the impact of hemodynamic factors on the outcome.
Methods: We reviewed the records of patients with a diagnosis of PH admitted to the intensive care unit. In addition to evaluating traditional hemodynamic parameters, we defined severe PH as right atrial pressure >20 mmHg, mean pulmonary artery pressure >55 mmHg, or cardiac index (CI) <2 L/min/m(2). We also defined the RV functional index (RFI) as pulmonary artery systolic pressure (PASP) adjusted for CI as PASP/CI; increasing values reflect RV dysfunction.
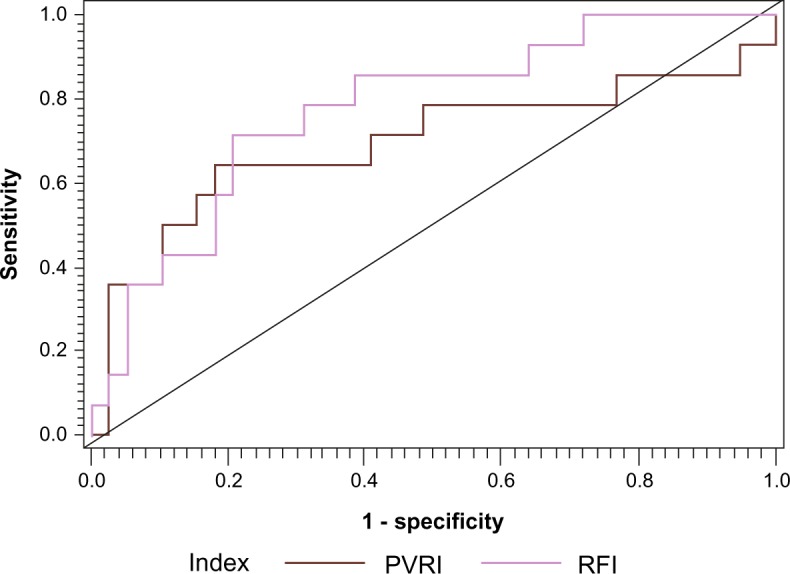
Results: Fifty-three patients (mean age 60 years, 72% women, 79% Blacks), were included in the study. Severe PH was present in 68% of patients who had higher Sequential Organ Failure Assessment (SOFA) score (6.8 ± 3.3 vs 3.8 ± 1.6; P = 0.001) and overall in-hospital mortality (36% vs 6%; P = 0.02) compared to nonsevere patients, although Acute Physiology and Chronic Health Evaluation (APACHE) II scores (19.9 ± 7.5 vs 18.5 ± 6.04; P = 0.52) were similar and sepsis was more frequent among nonsevere PH patients (31 vs 64%; P = 0.02). Severe PH (P = 0.04), lower mean arterial pressure (P = 0.04), and CI (P = 0.01); need for invasive ventilation (P = 0.02) and vasopressors (P = 0.03); and higher SOFA (P = 0.001), APACHE II (P = 0.03), pulmonary vascular resistance index (PVRI) (P = 0.01), and RFI (P = 0.004) were associated with increased mortality. In a multivariate model, SOFA [OR = 1.45, 95% confidence interval (C.I.) = 1.09-1.93; P = 0.01], PVRI (OR = 1.12, 95% C.I. = 1.02-1.24; P = 0.02), and increasing RFI (OR = 1.06, 95% C.I. = 1.01-1.11; P = 0.01) were independently associated with mortality.
Conclusion: PH is an independent risk factor for mortality in critically ill patients. Composite factors rather than individual hemodynamic parameters are better predictors of outcome. Monitoring of RV function using composite hemodynamic factors resulting in specific interventions is likely to improve survival and needs to be studied further.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


