{"title":"基于植入棒变形的脊柱侧凸矫正力的三维有限元分析。","authors":"Yuichiro Abe, Manabu Ito, Kuniyoshi Abumi, Hideki Sudo, Remel Salmingo, Shigeru Tadano","doi":"10.1186/1748-7161-10-S2-S2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Improvement of material property in spinal instrumentation has brought better deformity correction in scoliosis surgery in recent years. The increase of mechanical strength in instruments directly means the increase of force, which acts on bone-implant interface during scoliosis surgery. However, the actual correction force during the correction maneuver and safety margin of pull out force on each screw were not well known. In the present study, estimated corrective forces and pull out forces were analyzed using a novel method based on Finite Element Analysis (FEA).</p><p><strong>Methods: </strong>Twenty adolescent idiopathic scoliosis patients (1 boy and 19 girls) who underwent reconstructive scoliosis surgery between June 2009 and Jun 2011 were included in this study. Scoliosis correction was performed with 6mm diameter titanium rod (Ti6Al7Nb) using the simultaneous double rod rotation technique (SDRRT) in all cases. The pre-maneuver and post-maneuver rod geometry was collected from intraoperative tracing and postoperative 3D-CT images, and 3D-FEA was performed with ANSYS. Cobb angle of major curve, correction rate and thoracic kyphosis were measured on X-ray images.</p><p><strong>Results: </strong>Average age at surgery was 14.8, and average fusion length was 8.9 segments. Major curve was corrected from 63.1 to 18.1 degrees in average and correction rate was 71.4%. Rod geometry showed significant change on the concave side. Curvature of the rod on concave and convex sides decreased from 33.6 to 17.8 degrees, and from 25.9 to 23.8 degrees, respectively. Estimated pull out forces at apical vertebrae were 160.0N in the concave side screw and 35.6N in the convex side screw. Estimated push in force at LIV and UIV were 305.1N in the concave side screw and 86.4N in the convex side screw.</p><p><strong>Conclusions: </strong>Corrective force during scoliosis surgery was demonstrated to be about four times greater in the concave side than in convex side. Averaged pull out and push in force fell below previously reported safety margin. Therefore, the SDRRT maneuver was safe for correcting moderate magnitude curves. To prevent implant breakage or pedicle fracture during the maneuver in a severe curve correction, mobilization of spinal segment by releasing soft tissue or facet joint could be more important than using a stronger correction maneuver with a rigid implant.</p>","PeriodicalId":21722,"journal":{"name":"Scoliosis","volume":"10 Suppl 2","pages":"S2"},"PeriodicalIF":0.0000,"publicationDate":"2015-02-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/1748-7161-10-S2-S2","citationCount":"25","resultStr":"{\"title\":\"Scoliosis corrective force estimation from the implanted rod deformation using 3D-FEM analysis.\",\"authors\":\"Yuichiro Abe, Manabu Ito, Kuniyoshi Abumi, Hideki Sudo, Remel Salmingo, Shigeru Tadano\",\"doi\":\"10.1186/1748-7161-10-S2-S2\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Improvement of material property in spinal instrumentation has brought better deformity correction in scoliosis surgery in recent years. The increase of mechanical strength in instruments directly means the increase of force, which acts on bone-implant interface during scoliosis surgery. However, the actual correction force during the correction maneuver and safety margin of pull out force on each screw were not well known. In the present study, estimated corrective forces and pull out forces were analyzed using a novel method based on Finite Element Analysis (FEA).</p><p><strong>Methods: </strong>Twenty adolescent idiopathic scoliosis patients (1 boy and 19 girls) who underwent reconstructive scoliosis surgery between June 2009 and Jun 2011 were included in this study. Scoliosis correction was performed with 6mm diameter titanium rod (Ti6Al7Nb) using the simultaneous double rod rotation technique (SDRRT) in all cases. The pre-maneuver and post-maneuver rod geometry was collected from intraoperative tracing and postoperative 3D-CT images, and 3D-FEA was performed with ANSYS. Cobb angle of major curve, correction rate and thoracic kyphosis were measured on X-ray images.</p><p><strong>Results: </strong>Average age at surgery was 14.8, and average fusion length was 8.9 segments. Major curve was corrected from 63.1 to 18.1 degrees in average and correction rate was 71.4%. Rod geometry showed significant change on the concave side. Curvature of the rod on concave and convex sides decreased from 33.6 to 17.8 degrees, and from 25.9 to 23.8 degrees, respectively. Estimated pull out forces at apical vertebrae were 160.0N in the concave side screw and 35.6N in the convex side screw. Estimated push in force at LIV and UIV were 305.1N in the concave side screw and 86.4N in the convex side screw.</p><p><strong>Conclusions: </strong>Corrective force during scoliosis surgery was demonstrated to be about four times greater in the concave side than in convex side. Averaged pull out and push in force fell below previously reported safety margin. Therefore, the SDRRT maneuver was safe for correcting moderate magnitude curves. To prevent implant breakage or pedicle fracture during the maneuver in a severe curve correction, mobilization of spinal segment by releasing soft tissue or facet joint could be more important than using a stronger correction maneuver with a rigid implant.</p>\",\"PeriodicalId\":21722,\"journal\":{\"name\":\"Scoliosis\",\"volume\":\"10 Suppl 2\",\"pages\":\"S2\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2015-02-11\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1186/1748-7161-10-S2-S2\",\"citationCount\":\"25\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Scoliosis\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/1748-7161-10-S2-S2\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2015/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Scoliosis","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/1748-7161-10-S2-S2","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2015/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Scoliosis corrective force estimation from the implanted rod deformation using 3D-FEM analysis.
Background: Improvement of material property in spinal instrumentation has brought better deformity correction in scoliosis surgery in recent years. The increase of mechanical strength in instruments directly means the increase of force, which acts on bone-implant interface during scoliosis surgery. However, the actual correction force during the correction maneuver and safety margin of pull out force on each screw were not well known. In the present study, estimated corrective forces and pull out forces were analyzed using a novel method based on Finite Element Analysis (FEA).
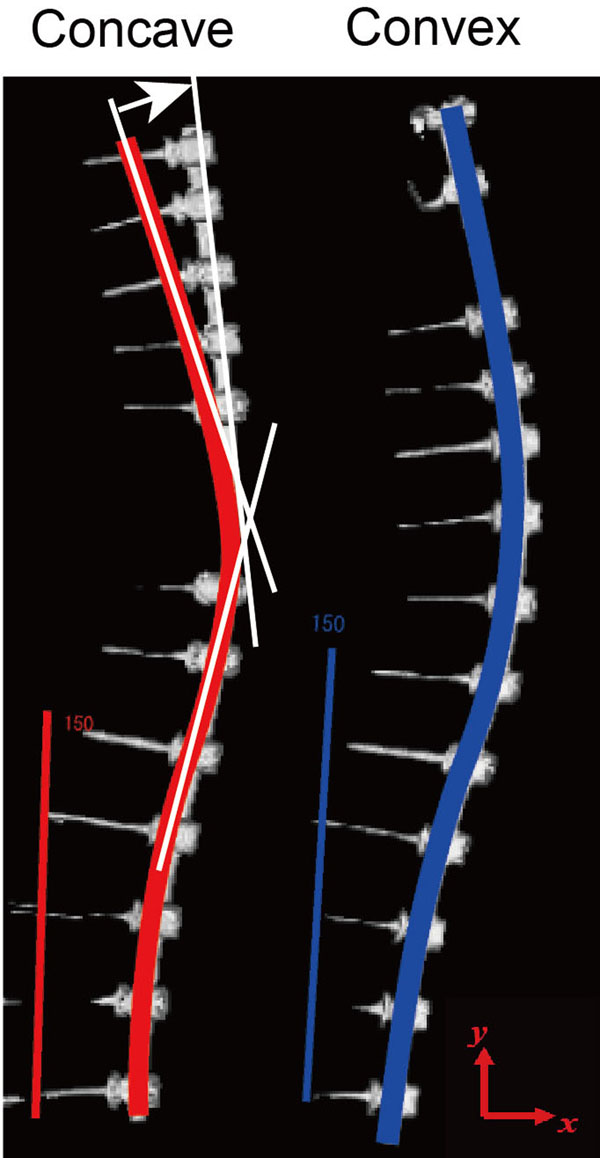
Methods: Twenty adolescent idiopathic scoliosis patients (1 boy and 19 girls) who underwent reconstructive scoliosis surgery between June 2009 and Jun 2011 were included in this study. Scoliosis correction was performed with 6mm diameter titanium rod (Ti6Al7Nb) using the simultaneous double rod rotation technique (SDRRT) in all cases. The pre-maneuver and post-maneuver rod geometry was collected from intraoperative tracing and postoperative 3D-CT images, and 3D-FEA was performed with ANSYS. Cobb angle of major curve, correction rate and thoracic kyphosis were measured on X-ray images.
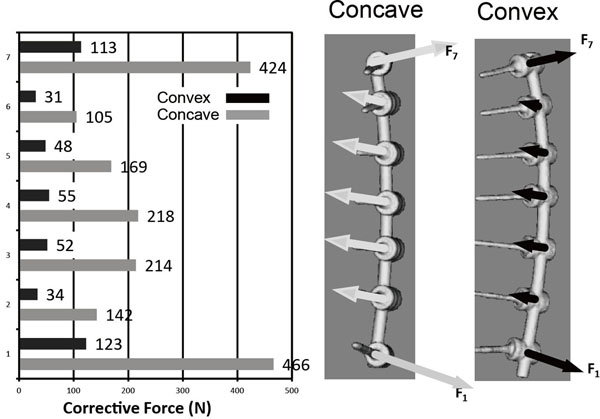
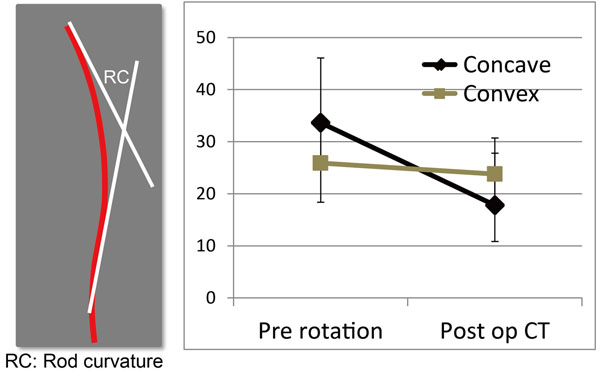
Results: Average age at surgery was 14.8, and average fusion length was 8.9 segments. Major curve was corrected from 63.1 to 18.1 degrees in average and correction rate was 71.4%. Rod geometry showed significant change on the concave side. Curvature of the rod on concave and convex sides decreased from 33.6 to 17.8 degrees, and from 25.9 to 23.8 degrees, respectively. Estimated pull out forces at apical vertebrae were 160.0N in the concave side screw and 35.6N in the convex side screw. Estimated push in force at LIV and UIV were 305.1N in the concave side screw and 86.4N in the convex side screw.
Conclusions: Corrective force during scoliosis surgery was demonstrated to be about four times greater in the concave side than in convex side. Averaged pull out and push in force fell below previously reported safety margin. Therefore, the SDRRT maneuver was safe for correcting moderate magnitude curves. To prevent implant breakage or pedicle fracture during the maneuver in a severe curve correction, mobilization of spinal segment by releasing soft tissue or facet joint could be more important than using a stronger correction maneuver with a rigid implant.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


