{"title":"儿童鼻腔和副鼻窦疾病。","authors":"Markus Stenner, Claudia Rudack","doi":"10.3205/cto000113","DOIUrl":null,"url":null,"abstract":"<p><p>Diseases of the pediatric nose and nasal sinuses as well as neighboring anatomical structures encompass a variety of pathologies, especially of inflammatory nature. Congenital disease, such as malformations and structural deviations of the nasal septum, as well as systemic metabolic pathologies affecting the nose and sinuses, rarely require medical therapy from an Otolaryngologist. The immunological function of the mucosa and genetic factors play a role in the development of disease in the pediatric upper airway tract, especially due to the constantly changing anatomy in this growth phase. Disease description of the nose and nasal sinuses due to mid-facial growth must also take developmental age differences (infant, toddler, preschool, and school age) into account. Epidemiological examinations and evidence based studies are often lacking in the pediatric population. The wide range of inflammatory diseases of the nose and paranasal sinuses, such as the acute and chronic rhinosinusitis, the allergic rhinitis, and adenoid disease, play a role in the susceptibility of a child to infection. The susceptibility to infection depends on the pediatric age structure (infant, young child) and has yet to be well defined. The acute rhinosinusitis in children develops after a viral infection of the upper airways, also referred to as the \"common cold\" in the literature. It usually spontaneously heals within ten days without any medical therapy. Antibiotic therapy is prudent in complicated episodes of ARS. The antibiotic therapy is reserved for children with complications or associated disease, such as bronchial asthma and/or chronic bronchitis. A chronic rhinosinusitis is defined as the inflammatory change in the nasal mucosa and nasal sinus mucosa, in which the corresponding symptoms persist for over 12 weeks. The indication for CT-imaging of the nasal sinuses is reserved for cases of chronic rhinosinusitis that have been successfully treated with medication. A staged therapeutic concept is followed in CRS based on conservative and surgical methods. Nasal sinus surgery is considered nowadays as effective and safe in children. Based on the assumption that adenoids are a reservoir for bacteria, from which recurrent infections of the nose and nasal sinus originate, the adenoidectomy is still defined as a cleansing procedure in rhinosinusitis. 69.3% of the children had benefit from adenoidectomy. Comorbidities, such as pediatric bronchial asthma, presently play an even more important role in the therapy of rhinosinusitis; therefore, it is often wise to have the support of pediatricians. In western European countries 40% of children presently suffer from allergic rhinitis, in which pronounced nasal obstruction can cause disturbed growth in facial bones. An early therapy with SIT may prevent the development of bronchial asthma and secondary sensitization to other allergens. Therefore, SIT is recommended in treatment of allergic rhinitis whenever, if possible. The assessment of diagnostic tools is for the examiner not often possible due to the lack of evidence. Rhinosurgical approaches are often described in study reports; however, they lack the standard prospective randomized long-term study design required nowadays and can only be evaluated with caution in the literature. </p>","PeriodicalId":89377,"journal":{"name":"GMS current topics in otorhinolaryngology, head and neck surgery","volume":"13 ","pages":"Doc10"},"PeriodicalIF":0.0000,"publicationDate":"2014-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/c4/b4/CTO-13-10.PMC4273171.pdf","citationCount":"0","resultStr":"{\"title\":\"Diseases of the nose and paranasal sinuses in child.\",\"authors\":\"Markus Stenner, Claudia Rudack\",\"doi\":\"10.3205/cto000113\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Diseases of the pediatric nose and nasal sinuses as well as neighboring anatomical structures encompass a variety of pathologies, especially of inflammatory nature. Congenital disease, such as malformations and structural deviations of the nasal septum, as well as systemic metabolic pathologies affecting the nose and sinuses, rarely require medical therapy from an Otolaryngologist. The immunological function of the mucosa and genetic factors play a role in the development of disease in the pediatric upper airway tract, especially due to the constantly changing anatomy in this growth phase. Disease description of the nose and nasal sinuses due to mid-facial growth must also take developmental age differences (infant, toddler, preschool, and school age) into account. Epidemiological examinations and evidence based studies are often lacking in the pediatric population. The wide range of inflammatory diseases of the nose and paranasal sinuses, such as the acute and chronic rhinosinusitis, the allergic rhinitis, and adenoid disease, play a role in the susceptibility of a child to infection. The susceptibility to infection depends on the pediatric age structure (infant, young child) and has yet to be well defined. The acute rhinosinusitis in children develops after a viral infection of the upper airways, also referred to as the \\\"common cold\\\" in the literature. It usually spontaneously heals within ten days without any medical therapy. Antibiotic therapy is prudent in complicated episodes of ARS. The antibiotic therapy is reserved for children with complications or associated disease, such as bronchial asthma and/or chronic bronchitis. A chronic rhinosinusitis is defined as the inflammatory change in the nasal mucosa and nasal sinus mucosa, in which the corresponding symptoms persist for over 12 weeks. The indication for CT-imaging of the nasal sinuses is reserved for cases of chronic rhinosinusitis that have been successfully treated with medication. A staged therapeutic concept is followed in CRS based on conservative and surgical methods. Nasal sinus surgery is considered nowadays as effective and safe in children. Based on the assumption that adenoids are a reservoir for bacteria, from which recurrent infections of the nose and nasal sinus originate, the adenoidectomy is still defined as a cleansing procedure in rhinosinusitis. 69.3% of the children had benefit from adenoidectomy. Comorbidities, such as pediatric bronchial asthma, presently play an even more important role in the therapy of rhinosinusitis; therefore, it is often wise to have the support of pediatricians. In western European countries 40% of children presently suffer from allergic rhinitis, in which pronounced nasal obstruction can cause disturbed growth in facial bones. An early therapy with SIT may prevent the development of bronchial asthma and secondary sensitization to other allergens. Therefore, SIT is recommended in treatment of allergic rhinitis whenever, if possible. The assessment of diagnostic tools is for the examiner not often possible due to the lack of evidence. Rhinosurgical approaches are often described in study reports; however, they lack the standard prospective randomized long-term study design required nowadays and can only be evaluated with caution in the literature. </p>\",\"PeriodicalId\":89377,\"journal\":{\"name\":\"GMS current topics in otorhinolaryngology, head and neck surgery\",\"volume\":\"13 \",\"pages\":\"Doc10\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2014-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/c4/b4/CTO-13-10.PMC4273171.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"GMS current topics in otorhinolaryngology, head and neck surgery\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3205/cto000113\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2014/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"GMS current topics in otorhinolaryngology, head and neck surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3205/cto000113","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2014/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
小儿鼻子和鼻窦以及邻近解剖结构的疾病包括各种病症,尤其是炎症性病症。先天性疾病,如鼻中隔畸形和结构偏差,以及影响鼻子和鼻窦的全身代谢性病变,很少需要耳鼻喉科医生的药物治疗。粘膜的免疫功能和遗传因素在小儿上呼吸道疾病的发生发展中起着重要作用,特别是由于在这一生长阶段解剖结构不断变化。在描述鼻腔和鼻窦因面中部生长而引起的疾病时,还必须考虑到发育年龄的差异(婴儿、幼儿、学龄前儿童和学龄儿童)。儿科人群往往缺乏流行病学检查和循证研究。鼻腔和副鼻窦的炎症性疾病种类繁多,如急性和慢性鼻炎、过敏性鼻炎和腺样体疾病等,这些都是导致儿童易受感染的原因之一。感染的易感性取决于儿童的年龄结构(婴儿、幼儿),目前还没有明确的定义。儿童急性鼻炎是在上呼吸道受到病毒感染后发生的,文献中也称之为 "普通感冒"。通常无需任何药物治疗即可在十天内自愈。对于复杂的 ARS 病例,应谨慎使用抗生素治疗。抗生素治疗适用于有并发症或相关疾病(如支气管哮喘和/或慢性支气管炎)的儿童。慢性鼻炎的定义是鼻粘膜和鼻窦粘膜发生炎症性改变,且相应症状持续 12 周以上。鼻窦 CT 扫描的适应症仅限于药物治疗成功的慢性鼻炎病例。CRS 采用分阶段治疗理念,以保守治疗和手术治疗为基础。如今,鼻窦手术在儿童中被认为是有效和安全的。腺样体是细菌的贮藏库,鼻腔和鼻窦的反复感染就源于腺样体,基于这一假设,腺样体切除术仍被定义为鼻窦炎的清洁手术。69.3%的儿童从腺样体切除术中获益。合并症,如小儿支气管哮喘,目前在鼻炎治疗中扮演着更加重要的角色;因此,得到儿科医生的支持通常是明智之举。在西欧国家,目前有 40% 的儿童患有过敏性鼻炎,明显的鼻腔阻塞会导致面部骨骼发育不良。早期使用 SIT 治疗可预防支气管哮喘的发展和对其他过敏原的继发性过敏。因此,如果可能,建议在治疗过敏性鼻炎时使用 SIT。由于缺乏证据,检查者往往无法对诊断工具进行评估。研究报告中经常描述鼻外科手术方法,但这些方法缺乏当今所需的标准前瞻性随机长期研究设计,因此只能在文献中谨慎评估。
Diseases of the nose and paranasal sinuses in child.
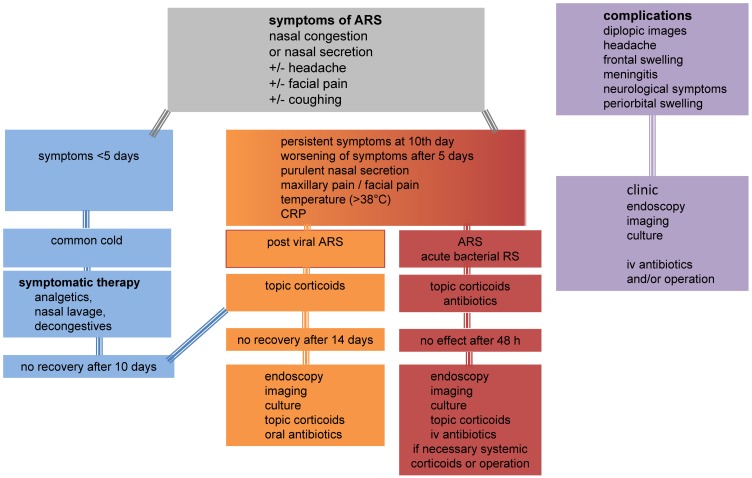
Diseases of the pediatric nose and nasal sinuses as well as neighboring anatomical structures encompass a variety of pathologies, especially of inflammatory nature. Congenital disease, such as malformations and structural deviations of the nasal septum, as well as systemic metabolic pathologies affecting the nose and sinuses, rarely require medical therapy from an Otolaryngologist. The immunological function of the mucosa and genetic factors play a role in the development of disease in the pediatric upper airway tract, especially due to the constantly changing anatomy in this growth phase. Disease description of the nose and nasal sinuses due to mid-facial growth must also take developmental age differences (infant, toddler, preschool, and school age) into account. Epidemiological examinations and evidence based studies are often lacking in the pediatric population. The wide range of inflammatory diseases of the nose and paranasal sinuses, such as the acute and chronic rhinosinusitis, the allergic rhinitis, and adenoid disease, play a role in the susceptibility of a child to infection. The susceptibility to infection depends on the pediatric age structure (infant, young child) and has yet to be well defined. The acute rhinosinusitis in children develops after a viral infection of the upper airways, also referred to as the "common cold" in the literature. It usually spontaneously heals within ten days without any medical therapy. Antibiotic therapy is prudent in complicated episodes of ARS. The antibiotic therapy is reserved for children with complications or associated disease, such as bronchial asthma and/or chronic bronchitis. A chronic rhinosinusitis is defined as the inflammatory change in the nasal mucosa and nasal sinus mucosa, in which the corresponding symptoms persist for over 12 weeks. The indication for CT-imaging of the nasal sinuses is reserved for cases of chronic rhinosinusitis that have been successfully treated with medication. A staged therapeutic concept is followed in CRS based on conservative and surgical methods. Nasal sinus surgery is considered nowadays as effective and safe in children. Based on the assumption that adenoids are a reservoir for bacteria, from which recurrent infections of the nose and nasal sinus originate, the adenoidectomy is still defined as a cleansing procedure in rhinosinusitis. 69.3% of the children had benefit from adenoidectomy. Comorbidities, such as pediatric bronchial asthma, presently play an even more important role in the therapy of rhinosinusitis; therefore, it is often wise to have the support of pediatricians. In western European countries 40% of children presently suffer from allergic rhinitis, in which pronounced nasal obstruction can cause disturbed growth in facial bones. An early therapy with SIT may prevent the development of bronchial asthma and secondary sensitization to other allergens. Therefore, SIT is recommended in treatment of allergic rhinitis whenever, if possible. The assessment of diagnostic tools is for the examiner not often possible due to the lack of evidence. Rhinosurgical approaches are often described in study reports; however, they lack the standard prospective randomized long-term study design required nowadays and can only be evaluated with caution in the literature.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


