Renee L Arlow, Dirk F Moore, Chunxia Chen, John Langenfeld, David A August
{"title":"结果-容量关系和经食管切除术:尽量减少“抢救失败”。","authors":"Renee L Arlow, Dirk F Moore, Chunxia Chen, John Langenfeld, David A August","doi":"10.1186/s13022-014-0009-3","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The objective of this study is to describe the system and technical factors that enabled our moderate size transhiatal esophagectomy program to achieve low mortality rates.</p><p><strong>Methods: </strong>A retrospective chart review was conducted on 200 consecutive patients who underwent transhiatal esophagectomy at Robert Wood Johnson University Hospital. Primary outcomes included operative times, estimated blood loss, frequency and nature of complications, and lengths of stay in the hospital and the intensive care unit.</p><p><strong>Results: </strong>In general, surgical outcomes tended to improve over the course of this study. We identified decreased operative time, intra-operative blood loss, frequency of complications, and lengths of intensive care unit and hospital stay as the program matured. Through coordinated actions of the surgical and anesthesia teams, all intraoperative injuries were responded to in an effective, emergent fashion and all but one patient was saved. This resulted in an inhospital and 30-day mortality rate of only 0.5%.</p><p><strong>Conclusions: </strong>Our study suggests that a dual attending approach, focus on avoiding \"failure to rescue\", increased volume, and a surgeon driven commitment to quality improvement may lead to low mortality rates after transhiatal esophagectomy.</p>","PeriodicalId":87428,"journal":{"name":"Annals of surgical innovation and research","volume":"8 1","pages":"9"},"PeriodicalIF":0.0000,"publicationDate":"2014-12-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/s13022-014-0009-3","citationCount":"11","resultStr":"{\"title\":\"Outcome-volume relationships and transhiatal esophagectomy: minimizing \\\"failure to rescue\\\".\",\"authors\":\"Renee L Arlow, Dirk F Moore, Chunxia Chen, John Langenfeld, David A August\",\"doi\":\"10.1186/s13022-014-0009-3\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The objective of this study is to describe the system and technical factors that enabled our moderate size transhiatal esophagectomy program to achieve low mortality rates.</p><p><strong>Methods: </strong>A retrospective chart review was conducted on 200 consecutive patients who underwent transhiatal esophagectomy at Robert Wood Johnson University Hospital. Primary outcomes included operative times, estimated blood loss, frequency and nature of complications, and lengths of stay in the hospital and the intensive care unit.</p><p><strong>Results: </strong>In general, surgical outcomes tended to improve over the course of this study. We identified decreased operative time, intra-operative blood loss, frequency of complications, and lengths of intensive care unit and hospital stay as the program matured. Through coordinated actions of the surgical and anesthesia teams, all intraoperative injuries were responded to in an effective, emergent fashion and all but one patient was saved. This resulted in an inhospital and 30-day mortality rate of only 0.5%.</p><p><strong>Conclusions: </strong>Our study suggests that a dual attending approach, focus on avoiding \\\"failure to rescue\\\", increased volume, and a surgeon driven commitment to quality improvement may lead to low mortality rates after transhiatal esophagectomy.</p>\",\"PeriodicalId\":87428,\"journal\":{\"name\":\"Annals of surgical innovation and research\",\"volume\":\"8 1\",\"pages\":\"9\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2014-12-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1186/s13022-014-0009-3\",\"citationCount\":\"11\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of surgical innovation and research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s13022-014-0009-3\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2014/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of surgical innovation and research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13022-014-0009-3","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2014/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Outcome-volume relationships and transhiatal esophagectomy: minimizing "failure to rescue".
Background: The objective of this study is to describe the system and technical factors that enabled our moderate size transhiatal esophagectomy program to achieve low mortality rates.
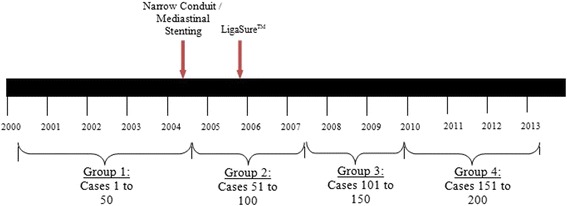
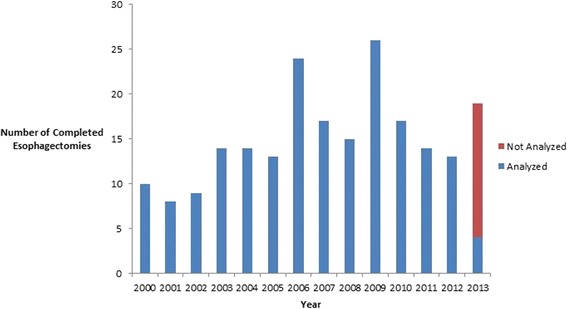
Methods: A retrospective chart review was conducted on 200 consecutive patients who underwent transhiatal esophagectomy at Robert Wood Johnson University Hospital. Primary outcomes included operative times, estimated blood loss, frequency and nature of complications, and lengths of stay in the hospital and the intensive care unit.
Results: In general, surgical outcomes tended to improve over the course of this study. We identified decreased operative time, intra-operative blood loss, frequency of complications, and lengths of intensive care unit and hospital stay as the program matured. Through coordinated actions of the surgical and anesthesia teams, all intraoperative injuries were responded to in an effective, emergent fashion and all but one patient was saved. This resulted in an inhospital and 30-day mortality rate of only 0.5%.
Conclusions: Our study suggests that a dual attending approach, focus on avoiding "failure to rescue", increased volume, and a surgeon driven commitment to quality improvement may lead to low mortality rates after transhiatal esophagectomy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


