Maxwell A Thompson, David T Redden, Lindsey Glueckert, A Blair Smith, Jack H Crawford, Keith A Jones, Devin E Eckhoff, Stephen H Gray, Jared A White, Joseph Bloomer, Derek A DuBay
{"title":"肝移植术后再手术出血的相关危险因素。","authors":"Maxwell A Thompson, David T Redden, Lindsey Glueckert, A Blair Smith, Jack H Crawford, Keith A Jones, Devin E Eckhoff, Stephen H Gray, Jared A White, Joseph Bloomer, Derek A DuBay","doi":"10.1155/2014/816246","DOIUrl":null,"url":null,"abstract":"<p><p>Introduction. This study's objective was to identify risk factors associated with reoperation for bleeding following liver transplantation (LTx). Methods. A retrospective study was performed at a single institution between 2001 and 2012. Operative reports were used to identify patients who underwent reoperation for bleeding within 2 weeks following LTx (operations for nonbleeding etiologies were excluded). Results. Reoperation for bleeding was observed in 101/928 (10.8%) of LTx patients. The following characteristics were associated with reoperation on multivariable analysis: recipient MELD score (OR 1.06/MELD unit, 95% CI 1.03, 1.09), number of platelets transfused (OR 0.73/platelet unit, 95% CI 0.58, 0.91), and aminocaproic acid utilization (OR 0.46, 95% CI 0.27, 0.80). LTx patients who underwent reoperation for bleeding had a longer ICU stay (5 days ± 7 versus 2 days ± 3, P < 0.001) and hospitalization (18 days ± 9 versus 10 days ± 18, P < 0.001). The risk of death increased in patients who underwent reoperation for bleeding (HR 1.89, 95% CI 1.26, 2.85). Conclusion. Reoperation for bleeding following LTx was associated with increased resource utilization and recipient mortality. A lower threshold for intraoperative platelet transfusion and antifibrinolytics, especially in patients with high lab-MELD score, may decrease the incidence of reoperation for bleeding following LTx. </p>","PeriodicalId":77165,"journal":{"name":"HPB surgery : a world journal of hepatic, pancreatic and biliary surgery","volume":"2014 ","pages":"816246"},"PeriodicalIF":0.0000,"publicationDate":"2014-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2014/816246","citationCount":"27","resultStr":"{\"title\":\"Risk Factors Associated with Reoperation for Bleeding following Liver Transplantation.\",\"authors\":\"Maxwell A Thompson, David T Redden, Lindsey Glueckert, A Blair Smith, Jack H Crawford, Keith A Jones, Devin E Eckhoff, Stephen H Gray, Jared A White, Joseph Bloomer, Derek A DuBay\",\"doi\":\"10.1155/2014/816246\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Introduction. This study's objective was to identify risk factors associated with reoperation for bleeding following liver transplantation (LTx). Methods. A retrospective study was performed at a single institution between 2001 and 2012. Operative reports were used to identify patients who underwent reoperation for bleeding within 2 weeks following LTx (operations for nonbleeding etiologies were excluded). Results. Reoperation for bleeding was observed in 101/928 (10.8%) of LTx patients. The following characteristics were associated with reoperation on multivariable analysis: recipient MELD score (OR 1.06/MELD unit, 95% CI 1.03, 1.09), number of platelets transfused (OR 0.73/platelet unit, 95% CI 0.58, 0.91), and aminocaproic acid utilization (OR 0.46, 95% CI 0.27, 0.80). LTx patients who underwent reoperation for bleeding had a longer ICU stay (5 days ± 7 versus 2 days ± 3, P < 0.001) and hospitalization (18 days ± 9 versus 10 days ± 18, P < 0.001). The risk of death increased in patients who underwent reoperation for bleeding (HR 1.89, 95% CI 1.26, 2.85). Conclusion. Reoperation for bleeding following LTx was associated with increased resource utilization and recipient mortality. A lower threshold for intraoperative platelet transfusion and antifibrinolytics, especially in patients with high lab-MELD score, may decrease the incidence of reoperation for bleeding following LTx. </p>\",\"PeriodicalId\":77165,\"journal\":{\"name\":\"HPB surgery : a world journal of hepatic, pancreatic and biliary surgery\",\"volume\":\"2014 \",\"pages\":\"816246\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2014-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1155/2014/816246\",\"citationCount\":\"27\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"HPB surgery : a world journal of hepatic, pancreatic and biliary surgery\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2014/816246\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2014/11/20 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"HPB surgery : a world journal of hepatic, pancreatic and biliary surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2014/816246","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2014/11/20 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 27
摘要
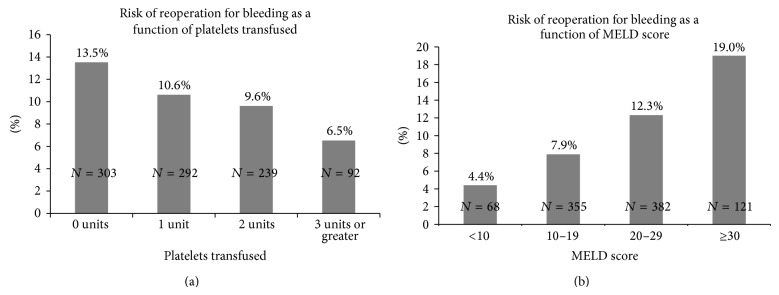
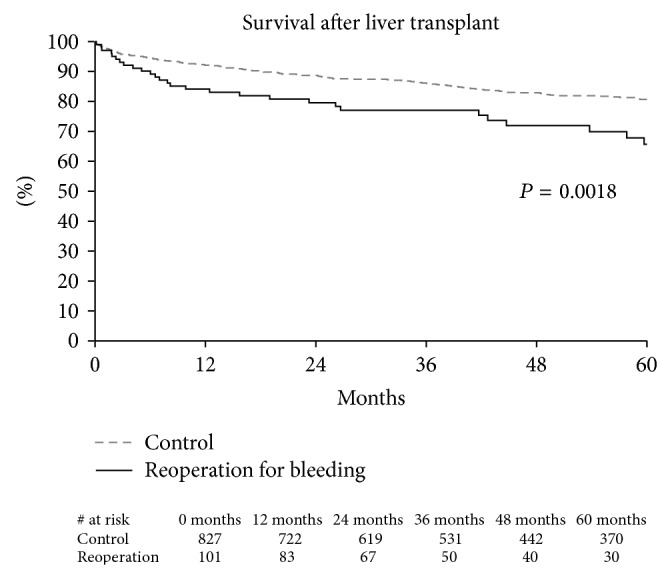
介绍。本研究的目的是确定与肝移植术后出血再手术相关的危险因素。方法。回顾性研究于2001年至2012年在一家机构进行。手术报告用于确定LTx术后2周内因出血再次手术的患者(排除非出血原因的手术)。结果。928例LTx患者中有101例(10.8%)因出血再次手术。在多变量分析中,以下特征与再手术相关:受体MELD评分(OR 1.06/MELD单位,95% CI 1.03, 1.09)、输血小板数(OR 0.73/血小板单位,95% CI 0.58, 0.91)和氨基自戊酸利用率(OR 0.46, 95% CI 0.27, 0.80)。因出血再手术的LTx患者在ICU的住院时间(5天±7天比2天±3天,P < 0.001)和住院时间(18天±9天比10天±18天,P < 0.001)更长。因出血再次手术的患者死亡风险增加(HR 1.89, 95% CI 1.26, 2.85)。结论。LTx术后出血再手术与资源利用率和受者死亡率增加有关。术中输注血小板和使用抗纤溶药物的阈值较低,尤其是实验室meld评分较高的患者,可能会降低LTx术后出血再手术的发生率。
Risk Factors Associated with Reoperation for Bleeding following Liver Transplantation.
Introduction. This study's objective was to identify risk factors associated with reoperation for bleeding following liver transplantation (LTx). Methods. A retrospective study was performed at a single institution between 2001 and 2012. Operative reports were used to identify patients who underwent reoperation for bleeding within 2 weeks following LTx (operations for nonbleeding etiologies were excluded). Results. Reoperation for bleeding was observed in 101/928 (10.8%) of LTx patients. The following characteristics were associated with reoperation on multivariable analysis: recipient MELD score (OR 1.06/MELD unit, 95% CI 1.03, 1.09), number of platelets transfused (OR 0.73/platelet unit, 95% CI 0.58, 0.91), and aminocaproic acid utilization (OR 0.46, 95% CI 0.27, 0.80). LTx patients who underwent reoperation for bleeding had a longer ICU stay (5 days ± 7 versus 2 days ± 3, P < 0.001) and hospitalization (18 days ± 9 versus 10 days ± 18, P < 0.001). The risk of death increased in patients who underwent reoperation for bleeding (HR 1.89, 95% CI 1.26, 2.85). Conclusion. Reoperation for bleeding following LTx was associated with increased resource utilization and recipient mortality. A lower threshold for intraoperative platelet transfusion and antifibrinolytics, especially in patients with high lab-MELD score, may decrease the incidence of reoperation for bleeding following LTx.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


