Jennifer A McCaughan, Christopher C Patterson, Alexander P Maxwell, Aisling E Courtney
{"title":"影响肾移植失败后生存的因素。","authors":"Jennifer A McCaughan, Christopher C Patterson, Alexander P Maxwell, Aisling E Courtney","doi":"10.1186/2047-1440-3-18","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The failure of a kidney transplant is now a common reason for initiation of dialysis therapy. Kidney transplant recipients commencing dialysis have greater morbidity and mortality than transplant-naïve, incident dialysis patients. This study aimed to identify variables associated with survival after graft failure.</p><p><strong>Methods: </strong>All recipients of first, deceased donor kidney transplants performed in Northern Ireland between 1986 and 2005 who had a functioning graft at 12 months were included (n = 585). Clinical and blood-derived variables (age, gender, primary renal disease, diabetic status, smoking status, human leukocyte antigen (HLA) mismatch, acute rejection episodes, immunosuppression, cardiovascular disease, graft survival, haemoglobin, albumin, phosphate, C reactive protein, estimated glomerular filtration rate (eGFR), rate of eGFR decline, dialysis modality, and access) were collected prospectively and investigated for association with re-transplantation and survival. The association between re-transplantation and survival was explored by modelling re-transplantation as a time-dependent covariate.</p><p><strong>Results: </strong>Median follow-up time was 12.1 years. Recipients with a failing graft (158/585) demonstrated rapid loss of eGFR prior to graft failure, reducing the time available to plan for alternative renal replacement therapy. Median survival after graft failure was 3.0 years. In multivariate analysis, age and re-transplantation were associated with survival after graft failure. Re-transplantation was associated with an 88% reduction in mortality.</p><p><strong>Conclusions: </strong>Optimal management of kidney transplant recipients with failing grafts requires early recognition of declining function and proactive preparation for re-transplantation given the substantial survival benefit this confers. The survival benefit associated with re-transplantation persists after prolonged exposure to immunosuppressive therapy.</p>","PeriodicalId":89864,"journal":{"name":"Transplantation research","volume":"3 ","pages":"18"},"PeriodicalIF":0.0000,"publicationDate":"2014-09-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/2047-1440-3-18","citationCount":"32","resultStr":"{\"title\":\"Factors influencing survival after kidney transplant failure.\",\"authors\":\"Jennifer A McCaughan, Christopher C Patterson, Alexander P Maxwell, Aisling E Courtney\",\"doi\":\"10.1186/2047-1440-3-18\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The failure of a kidney transplant is now a common reason for initiation of dialysis therapy. Kidney transplant recipients commencing dialysis have greater morbidity and mortality than transplant-naïve, incident dialysis patients. This study aimed to identify variables associated with survival after graft failure.</p><p><strong>Methods: </strong>All recipients of first, deceased donor kidney transplants performed in Northern Ireland between 1986 and 2005 who had a functioning graft at 12 months were included (n = 585). Clinical and blood-derived variables (age, gender, primary renal disease, diabetic status, smoking status, human leukocyte antigen (HLA) mismatch, acute rejection episodes, immunosuppression, cardiovascular disease, graft survival, haemoglobin, albumin, phosphate, C reactive protein, estimated glomerular filtration rate (eGFR), rate of eGFR decline, dialysis modality, and access) were collected prospectively and investigated for association with re-transplantation and survival. The association between re-transplantation and survival was explored by modelling re-transplantation as a time-dependent covariate.</p><p><strong>Results: </strong>Median follow-up time was 12.1 years. Recipients with a failing graft (158/585) demonstrated rapid loss of eGFR prior to graft failure, reducing the time available to plan for alternative renal replacement therapy. Median survival after graft failure was 3.0 years. In multivariate analysis, age and re-transplantation were associated with survival after graft failure. Re-transplantation was associated with an 88% reduction in mortality.</p><p><strong>Conclusions: </strong>Optimal management of kidney transplant recipients with failing grafts requires early recognition of declining function and proactive preparation for re-transplantation given the substantial survival benefit this confers. The survival benefit associated with re-transplantation persists after prolonged exposure to immunosuppressive therapy.</p>\",\"PeriodicalId\":89864,\"journal\":{\"name\":\"Transplantation research\",\"volume\":\"3 \",\"pages\":\"18\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2014-09-24\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1186/2047-1440-3-18\",\"citationCount\":\"32\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Transplantation research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/2047-1440-3-18\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2014/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Transplantation research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/2047-1440-3-18","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2014/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Factors influencing survival after kidney transplant failure.
Background: The failure of a kidney transplant is now a common reason for initiation of dialysis therapy. Kidney transplant recipients commencing dialysis have greater morbidity and mortality than transplant-naïve, incident dialysis patients. This study aimed to identify variables associated with survival after graft failure.
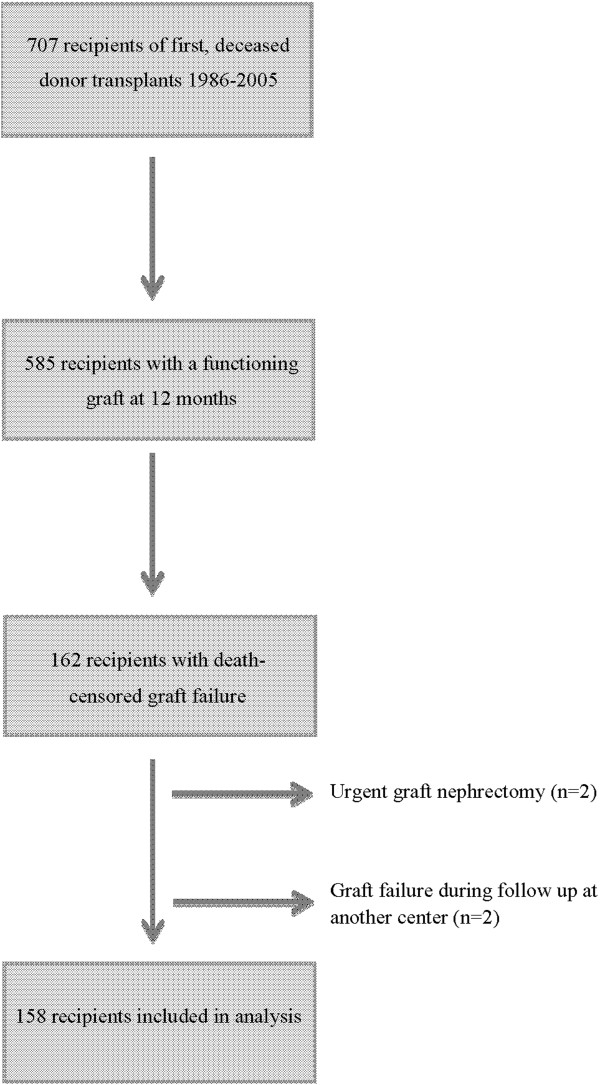
Methods: All recipients of first, deceased donor kidney transplants performed in Northern Ireland between 1986 and 2005 who had a functioning graft at 12 months were included (n = 585). Clinical and blood-derived variables (age, gender, primary renal disease, diabetic status, smoking status, human leukocyte antigen (HLA) mismatch, acute rejection episodes, immunosuppression, cardiovascular disease, graft survival, haemoglobin, albumin, phosphate, C reactive protein, estimated glomerular filtration rate (eGFR), rate of eGFR decline, dialysis modality, and access) were collected prospectively and investigated for association with re-transplantation and survival. The association between re-transplantation and survival was explored by modelling re-transplantation as a time-dependent covariate.
Results: Median follow-up time was 12.1 years. Recipients with a failing graft (158/585) demonstrated rapid loss of eGFR prior to graft failure, reducing the time available to plan for alternative renal replacement therapy. Median survival after graft failure was 3.0 years. In multivariate analysis, age and re-transplantation were associated with survival after graft failure. Re-transplantation was associated with an 88% reduction in mortality.
Conclusions: Optimal management of kidney transplant recipients with failing grafts requires early recognition of declining function and proactive preparation for re-transplantation given the substantial survival benefit this confers. The survival benefit associated with re-transplantation persists after prolonged exposure to immunosuppressive therapy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


