{"title":"慢性髓性白血病的治疗:伊马替尼时代的黄昏?","authors":"Ewelina Trela, Sylwester Glowacki, Janusz Błasiak","doi":"10.1155/2014/596483","DOIUrl":null,"url":null,"abstract":"<p><p>Chronic myeloid leukemia (CML) results from the clonal expansion of pluripotent hematopoietic stem cells containing the active BCR/ABL fusion gene produced by a reciprocal translocation of the ABL1 gene to the BCR gene. The BCR/ABL protein displays a constitutive tyrosine kinase activity and confers on leukemic cells growth and proliferation advantage and resistance to apoptosis. Introduction of imatinib (IM) and other tyrosine kinase inhibitors (TKIs) has radically improved the outcome of patients with CML and some other diseases with BCR/ABL expression. However, a fraction of CML patients presents with resistance to this drug. Regardless of clinical profits of IM, there are several drawbacks associated with its use, including lack of eradication of the malignant clone and increasing relapse rate resulting from long-term therapy, resistance, and intolerance. Second and third generations of TKIs have been developed to break IM resistance. Clinical studies revealed that the introduction of second-generation TKIs has improved the overall survival of CML patients; however, some with specific mutations such as T315I remain resistant. Second-generation TKIs may completely replace imatinib in perspective CML therapy, and addition of third-generation inhibitors may overcome resistance induced by every form of point mutations. </p>","PeriodicalId":89399,"journal":{"name":"ISRN oncology","volume":"2014 ","pages":"596483"},"PeriodicalIF":0.0000,"publicationDate":"2014-01-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2014/596483","citationCount":"38","resultStr":"{\"title\":\"Therapy of chronic myeloid leukemia: twilight of the imatinib era?\",\"authors\":\"Ewelina Trela, Sylwester Glowacki, Janusz Błasiak\",\"doi\":\"10.1155/2014/596483\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Chronic myeloid leukemia (CML) results from the clonal expansion of pluripotent hematopoietic stem cells containing the active BCR/ABL fusion gene produced by a reciprocal translocation of the ABL1 gene to the BCR gene. The BCR/ABL protein displays a constitutive tyrosine kinase activity and confers on leukemic cells growth and proliferation advantage and resistance to apoptosis. Introduction of imatinib (IM) and other tyrosine kinase inhibitors (TKIs) has radically improved the outcome of patients with CML and some other diseases with BCR/ABL expression. However, a fraction of CML patients presents with resistance to this drug. Regardless of clinical profits of IM, there are several drawbacks associated with its use, including lack of eradication of the malignant clone and increasing relapse rate resulting from long-term therapy, resistance, and intolerance. Second and third generations of TKIs have been developed to break IM resistance. Clinical studies revealed that the introduction of second-generation TKIs has improved the overall survival of CML patients; however, some with specific mutations such as T315I remain resistant. Second-generation TKIs may completely replace imatinib in perspective CML therapy, and addition of third-generation inhibitors may overcome resistance induced by every form of point mutations. </p>\",\"PeriodicalId\":89399,\"journal\":{\"name\":\"ISRN oncology\",\"volume\":\"2014 \",\"pages\":\"596483\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2014-01-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1155/2014/596483\",\"citationCount\":\"38\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"ISRN oncology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2014/596483\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2014/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"ISRN oncology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2014/596483","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2014/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Therapy of chronic myeloid leukemia: twilight of the imatinib era?
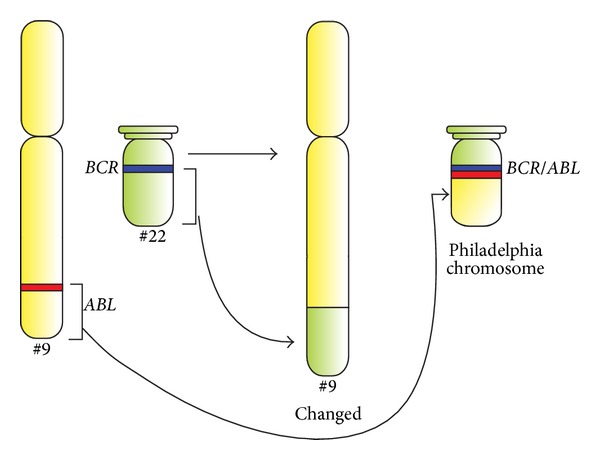
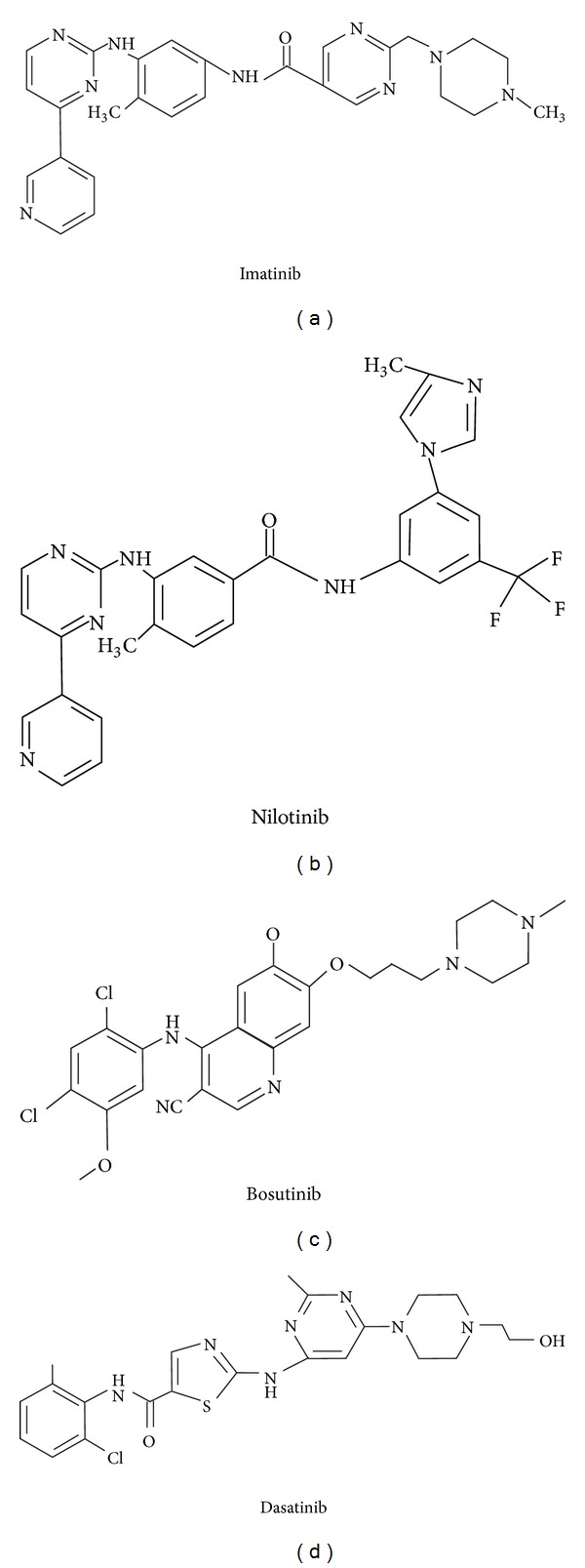
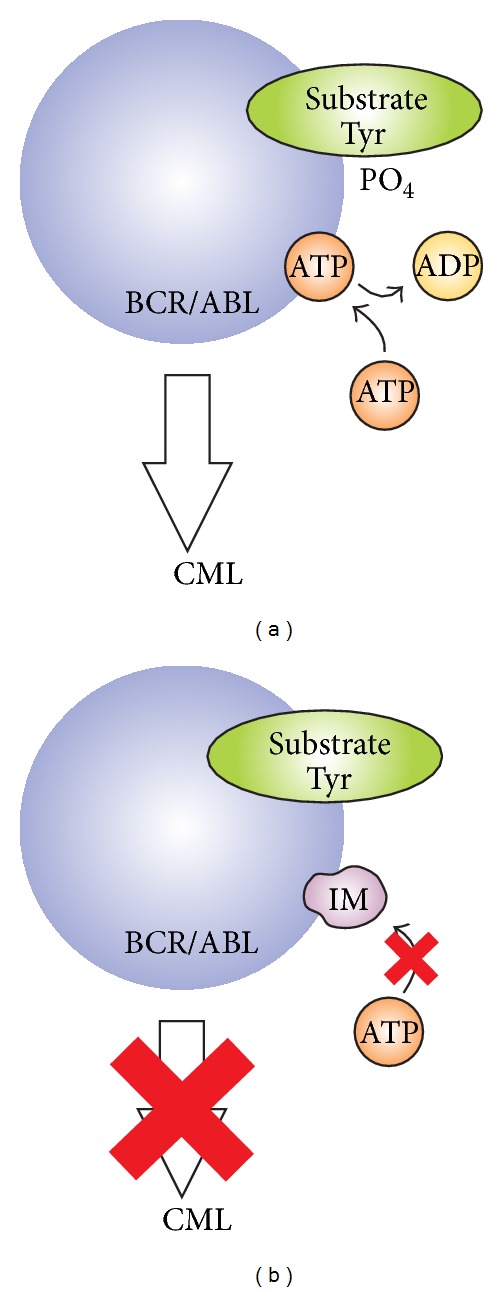
Chronic myeloid leukemia (CML) results from the clonal expansion of pluripotent hematopoietic stem cells containing the active BCR/ABL fusion gene produced by a reciprocal translocation of the ABL1 gene to the BCR gene. The BCR/ABL protein displays a constitutive tyrosine kinase activity and confers on leukemic cells growth and proliferation advantage and resistance to apoptosis. Introduction of imatinib (IM) and other tyrosine kinase inhibitors (TKIs) has radically improved the outcome of patients with CML and some other diseases with BCR/ABL expression. However, a fraction of CML patients presents with resistance to this drug. Regardless of clinical profits of IM, there are several drawbacks associated with its use, including lack of eradication of the malignant clone and increasing relapse rate resulting from long-term therapy, resistance, and intolerance. Second and third generations of TKIs have been developed to break IM resistance. Clinical studies revealed that the introduction of second-generation TKIs has improved the overall survival of CML patients; however, some with specific mutations such as T315I remain resistant. Second-generation TKIs may completely replace imatinib in perspective CML therapy, and addition of third-generation inhibitors may overcome resistance induced by every form of point mutations.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


