Fiona J Rowe, David Wright, Darren Brand, Carole Jackson, Shirley Harrison, Tallat Maan, Claire Scott, Linda Vogwell, Sarah Peel, Nicola Akerman, Caroline Dodridge, Claire Howard, Tracey Shipman, Una Sperring, Sonia Macdiarmid, Cicely Freeman
{"title":"脑血管意外后凝视功能障碍的概况。","authors":"Fiona J Rowe, David Wright, Darren Brand, Carole Jackson, Shirley Harrison, Tallat Maan, Claire Scott, Linda Vogwell, Sarah Peel, Nicola Akerman, Caroline Dodridge, Claire Howard, Tracey Shipman, Una Sperring, Sonia Macdiarmid, Cicely Freeman","doi":"10.1155/2013/264604","DOIUrl":null,"url":null,"abstract":"<p><p>Aim. To evaluate the profile of ocular gaze abnormalities occurring following stroke. Methods. Prospective multicentre cohort trial. Standardised referral and investigation protocol including assessment of visual acuity, ocular alignment and motility, visual field, and visual perception. Results. 915 patients recruited: mean age 69.18 years (SD 14.19). 498 patients (54%) were diagnosed with ocular motility abnormalities. 207 patients had gaze abnormalities including impaired gaze holding (46), complete gaze palsy (23), horizontal gaze palsy (16), vertical gaze palsy (17), Parinaud's syndrome (8), INO (20), one and half syndrome (3), saccadic palsy (28), and smooth pursuit palsy (46). These were isolated impairments in 50% of cases and in association with other ocular abnormalities in 50% including impaired convergence, nystagmus, and lid or pupil abnormalities. Areas of brain stroke were frequently the cerebellum, brainstem, and diencephalic areas. Strokes causing gaze dysfunction also involved cortical areas including occipital, parietal, and temporal lobes. Symptoms of diplopia and blurred vision were present in 35%. 37 patients were discharged, 29 referred, and 141 offered review appointments. 107 reviewed patients showed full recovery (4%), partial improvement (66%), and static gaze dysfunction (30%). Conclusions. Gaze dysfunction is common following stroke. Approximately one-third of patients complain of visual symptoms, two thirds show some improvement in ocular motility. </p>","PeriodicalId":90193,"journal":{"name":"ISRN ophthalmology","volume":"2013 ","pages":"264604"},"PeriodicalIF":0.0000,"publicationDate":"2013-10-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2013/264604","citationCount":"16","resultStr":"{\"title\":\"Profile of Gaze Dysfunction following Cerebrovascular Accident.\",\"authors\":\"Fiona J Rowe, David Wright, Darren Brand, Carole Jackson, Shirley Harrison, Tallat Maan, Claire Scott, Linda Vogwell, Sarah Peel, Nicola Akerman, Caroline Dodridge, Claire Howard, Tracey Shipman, Una Sperring, Sonia Macdiarmid, Cicely Freeman\",\"doi\":\"10.1155/2013/264604\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Aim. To evaluate the profile of ocular gaze abnormalities occurring following stroke. Methods. Prospective multicentre cohort trial. Standardised referral and investigation protocol including assessment of visual acuity, ocular alignment and motility, visual field, and visual perception. Results. 915 patients recruited: mean age 69.18 years (SD 14.19). 498 patients (54%) were diagnosed with ocular motility abnormalities. 207 patients had gaze abnormalities including impaired gaze holding (46), complete gaze palsy (23), horizontal gaze palsy (16), vertical gaze palsy (17), Parinaud's syndrome (8), INO (20), one and half syndrome (3), saccadic palsy (28), and smooth pursuit palsy (46). These were isolated impairments in 50% of cases and in association with other ocular abnormalities in 50% including impaired convergence, nystagmus, and lid or pupil abnormalities. Areas of brain stroke were frequently the cerebellum, brainstem, and diencephalic areas. Strokes causing gaze dysfunction also involved cortical areas including occipital, parietal, and temporal lobes. Symptoms of diplopia and blurred vision were present in 35%. 37 patients were discharged, 29 referred, and 141 offered review appointments. 107 reviewed patients showed full recovery (4%), partial improvement (66%), and static gaze dysfunction (30%). Conclusions. Gaze dysfunction is common following stroke. Approximately one-third of patients complain of visual symptoms, two thirds show some improvement in ocular motility. </p>\",\"PeriodicalId\":90193,\"journal\":{\"name\":\"ISRN ophthalmology\",\"volume\":\"2013 \",\"pages\":\"264604\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2013-10-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1155/2013/264604\",\"citationCount\":\"16\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"ISRN ophthalmology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2013/264604\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2013/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"ISRN ophthalmology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2013/264604","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2013/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Profile of Gaze Dysfunction following Cerebrovascular Accident.
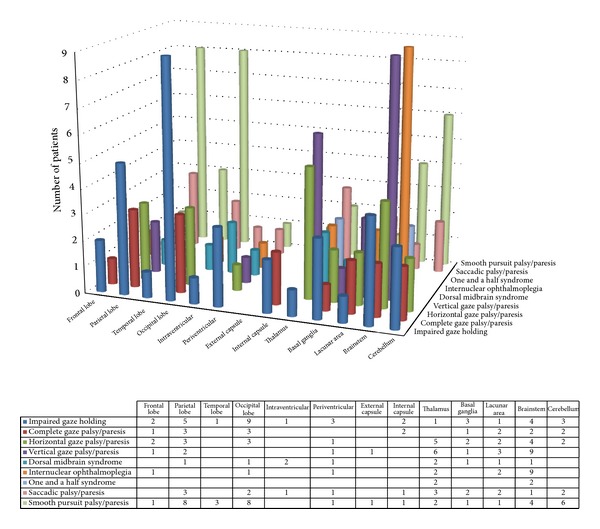
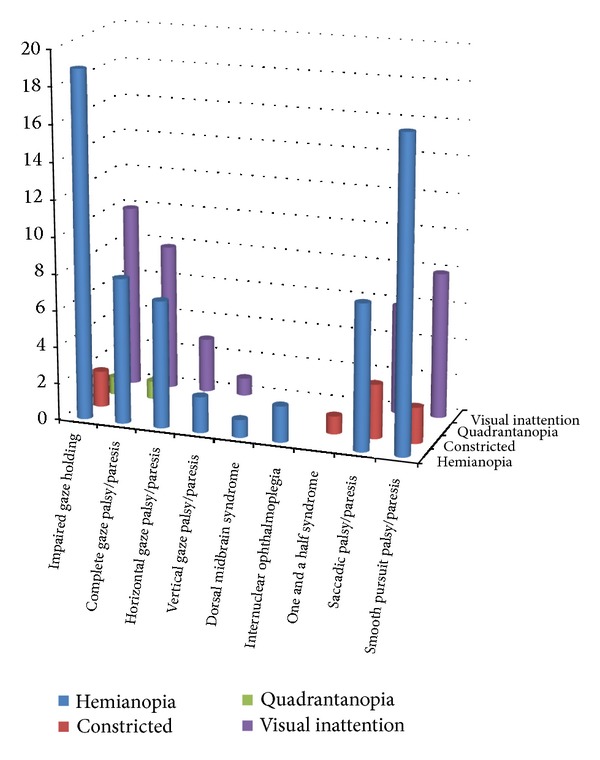
Aim. To evaluate the profile of ocular gaze abnormalities occurring following stroke. Methods. Prospective multicentre cohort trial. Standardised referral and investigation protocol including assessment of visual acuity, ocular alignment and motility, visual field, and visual perception. Results. 915 patients recruited: mean age 69.18 years (SD 14.19). 498 patients (54%) were diagnosed with ocular motility abnormalities. 207 patients had gaze abnormalities including impaired gaze holding (46), complete gaze palsy (23), horizontal gaze palsy (16), vertical gaze palsy (17), Parinaud's syndrome (8), INO (20), one and half syndrome (3), saccadic palsy (28), and smooth pursuit palsy (46). These were isolated impairments in 50% of cases and in association with other ocular abnormalities in 50% including impaired convergence, nystagmus, and lid or pupil abnormalities. Areas of brain stroke were frequently the cerebellum, brainstem, and diencephalic areas. Strokes causing gaze dysfunction also involved cortical areas including occipital, parietal, and temporal lobes. Symptoms of diplopia and blurred vision were present in 35%. 37 patients were discharged, 29 referred, and 141 offered review appointments. 107 reviewed patients showed full recovery (4%), partial improvement (66%), and static gaze dysfunction (30%). Conclusions. Gaze dysfunction is common following stroke. Approximately one-third of patients complain of visual symptoms, two thirds show some improvement in ocular motility.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


