{"title":"子宫切除术治疗生殖器脱垂的趋势:农村经验。","authors":"Shakuntala Chhabra, Manjiri Ramteke, Sonali Mehta, Nisha Bhole, Yojna Yadav","doi":"10.4137/CMRH.S10804","DOIUrl":null,"url":null,"abstract":"<p><p>The present study was conducted to investigate the trends of vaginal hysterectomy for genital prolapse in last 20 years by analyzing case records of affected women. During the analysis period, 4831 women underwent hysterectomy; records of 4223 (87.5%) were available. Of these, 911 (21.6%), 2.7% of 34,080 gynecological admissions, had vaginal hysterectomy for genital prolapse (study subjects). Eighty percent women who had vaginal hysterectomy for genital prolapse were over 40 years of age; however, most of these women had had the disorder for years before they presented. Only 4 (0.4%) women had not given birth, 874 (96%) women had had two or more births, and 383 (42%) had had 5 or more births. Having given birth was the major factor responsible for genital prolapse. In all, 94.2% of women presented with something coming out of the vagina.\" Some women presented with abnormal vaginal bleeding or pain in abdomen as the chief complaint although they had had uterovaginal prolapse for years. There was no mortality and morbidity decreased over the years. There has been no change in the rate of vaginal hysterectomy for genital prolapse over the years. Surgical morbidity decreased trend, possibly because of the preoperative, intraoperative, and postoperative precautions taken, especially preoperative treatment of urinary and genital tract infection. Attempts need to be made to have safe births and a healthy life style so as to prevent genital prolapse and in case it occurs, therapy to prevent progression so that major interventions like hysterectomy are averted. Meticulous preoperative evaluation and planned therapy help in reducing surgical morbidity, if surgery becomes essential. </p>","PeriodicalId":44130,"journal":{"name":"Clinical Medicine Insights-Reproductive Health","volume":"7 ","pages":"11-6"},"PeriodicalIF":0.0000,"publicationDate":"2013-01-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.4137/CMRH.S10804","citationCount":"2","resultStr":"{\"title\":\"Trends in hysterectomy for genital prolapse: rural experience.\",\"authors\":\"Shakuntala Chhabra, Manjiri Ramteke, Sonali Mehta, Nisha Bhole, Yojna Yadav\",\"doi\":\"10.4137/CMRH.S10804\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>The present study was conducted to investigate the trends of vaginal hysterectomy for genital prolapse in last 20 years by analyzing case records of affected women. During the analysis period, 4831 women underwent hysterectomy; records of 4223 (87.5%) were available. Of these, 911 (21.6%), 2.7% of 34,080 gynecological admissions, had vaginal hysterectomy for genital prolapse (study subjects). Eighty percent women who had vaginal hysterectomy for genital prolapse were over 40 years of age; however, most of these women had had the disorder for years before they presented. Only 4 (0.4%) women had not given birth, 874 (96%) women had had two or more births, and 383 (42%) had had 5 or more births. Having given birth was the major factor responsible for genital prolapse. In all, 94.2% of women presented with something coming out of the vagina.\\\" Some women presented with abnormal vaginal bleeding or pain in abdomen as the chief complaint although they had had uterovaginal prolapse for years. There was no mortality and morbidity decreased over the years. There has been no change in the rate of vaginal hysterectomy for genital prolapse over the years. Surgical morbidity decreased trend, possibly because of the preoperative, intraoperative, and postoperative precautions taken, especially preoperative treatment of urinary and genital tract infection. Attempts need to be made to have safe births and a healthy life style so as to prevent genital prolapse and in case it occurs, therapy to prevent progression so that major interventions like hysterectomy are averted. Meticulous preoperative evaluation and planned therapy help in reducing surgical morbidity, if surgery becomes essential. </p>\",\"PeriodicalId\":44130,\"journal\":{\"name\":\"Clinical Medicine Insights-Reproductive Health\",\"volume\":\"7 \",\"pages\":\"11-6\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2013-01-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.4137/CMRH.S10804\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Medicine Insights-Reproductive Health\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4137/CMRH.S10804\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine Insights-Reproductive Health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4137/CMRH.S10804","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Trends in hysterectomy for genital prolapse: rural experience.
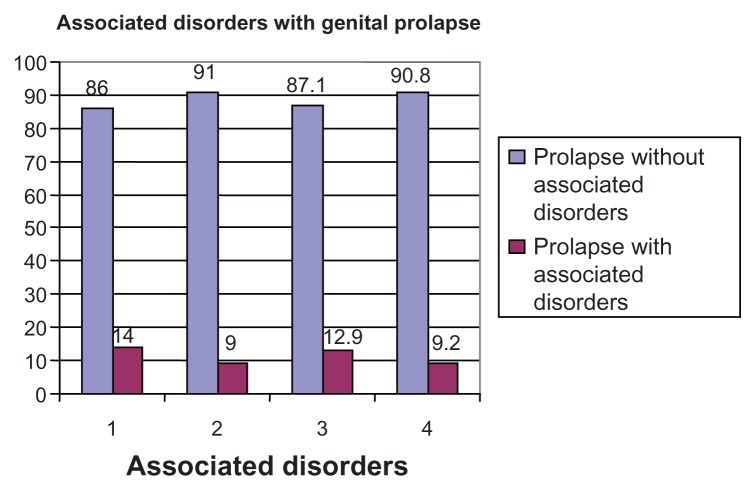
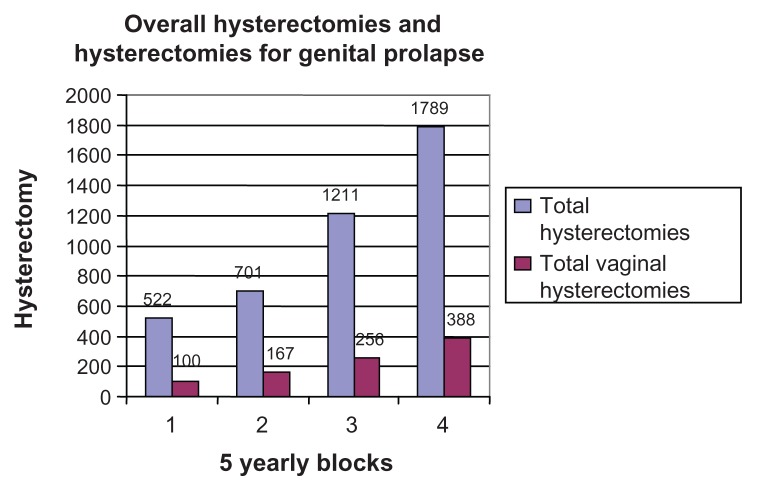
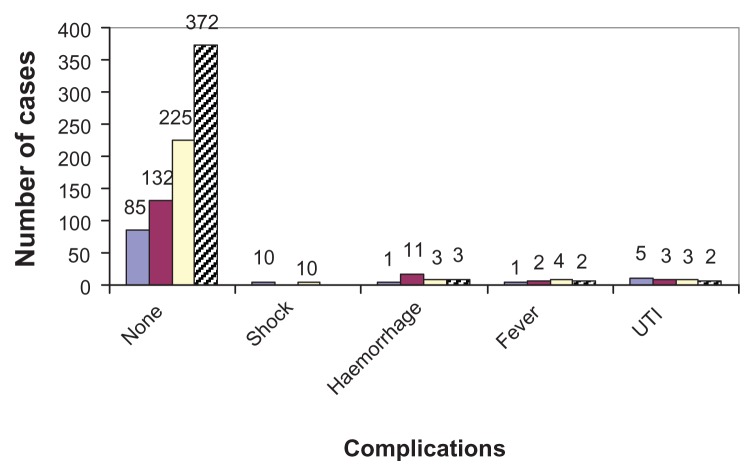
The present study was conducted to investigate the trends of vaginal hysterectomy for genital prolapse in last 20 years by analyzing case records of affected women. During the analysis period, 4831 women underwent hysterectomy; records of 4223 (87.5%) were available. Of these, 911 (21.6%), 2.7% of 34,080 gynecological admissions, had vaginal hysterectomy for genital prolapse (study subjects). Eighty percent women who had vaginal hysterectomy for genital prolapse were over 40 years of age; however, most of these women had had the disorder for years before they presented. Only 4 (0.4%) women had not given birth, 874 (96%) women had had two or more births, and 383 (42%) had had 5 or more births. Having given birth was the major factor responsible for genital prolapse. In all, 94.2% of women presented with something coming out of the vagina." Some women presented with abnormal vaginal bleeding or pain in abdomen as the chief complaint although they had had uterovaginal prolapse for years. There was no mortality and morbidity decreased over the years. There has been no change in the rate of vaginal hysterectomy for genital prolapse over the years. Surgical morbidity decreased trend, possibly because of the preoperative, intraoperative, and postoperative precautions taken, especially preoperative treatment of urinary and genital tract infection. Attempts need to be made to have safe births and a healthy life style so as to prevent genital prolapse and in case it occurs, therapy to prevent progression so that major interventions like hysterectomy are averted. Meticulous preoperative evaluation and planned therapy help in reducing surgical morbidity, if surgery becomes essential.
期刊介绍:
Clinical Medicine Insights: Reproductive Health is a peer reviewed; open access journal, which covers all aspects of Reproduction: Gynecology, Obstetrics, and Infertility, spanning both male and female issues, from the physical to the psychological and the social, including: sex, contraception, pregnancy, childbirth, and related topics such as social and emotional impacts. It welcomes original research and review articles from across the health sciences. Clinical subjects include fertility and sterility, infertility and assisted reproduction, IVF, fertility preservation despite gonadotoxic chemo- and/or radiotherapy, pregnancy problems, PPD, infections and disease, surgery, diagnosis, menopause, HRT, pelvic floor problems, reproductive cancers and environmental impacts on reproduction, although this list is by no means exhaustive Subjects covered include, but are not limited to: • fertility and sterility, • infertility and ART, • ART/IVF, • fertility preservation despite gonadotoxic chemo- and/or radiotherapy, • pregnancy problems, • Postpartum depression • Infections and disease, • Gyn/Ob surgery, • diagnosis, • Contraception • Premenstrual tension • Gynecologic Oncology • reproductive cancers • environmental impacts on reproduction, • Obstetrics/Gynaecology • Women''s Health • menopause, • HRT, • pelvic floor problems, • Paediatric and adolescent gynaecology • PID

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


