Reena Pattani, Valerie A Palda, Stephen W Hwang, Prakeshkumar S Shah
{"title":"益生菌预防住院患者抗生素相关性腹泻和艰难梭菌感染:系统评价和荟萃分析","authors":"Reena Pattani, Valerie A Palda, Stephen W Hwang, Prakeshkumar S Shah","doi":"","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Antibiotic-associated diarrhea (AAD) and Clostridium difficile infection (CDI) are associated with high morbidity, mortality, and health care costs. Probiotics may mitigate the existing disease burden. We performed a systematic review and meta-analysis to evaluate the efficacy of co-administration of probiotics with antibiotics in preventing these adverse outcomes in adult inpatients.</p><p><strong>Methods: </strong>Systematic searches of MEDLINE (1946 to May 2012), Embase (1980 to May 2012), and the Cochrane Central Register of Controlled Trials were undertaken on May 31, 2012, to identify relevant publications. We searched for randomized controlled trials, published in English, of adult inpatients who were receiving antibiotics and who were randomly assigned to co-administration of probiotics or usual care, with or without the use of placebo. Studies were included if they reported on AAD or CDI (or both) as outcomes. Data for predetermined criteria evaluating study characteristics, methods, and risk of bias were extracted. Trials were given a global rating of good, fair, or poor by at least 2 reviewers. Meta-analyses were performed using a random-effects model, and pooled relative risks (RRs) and 95% confidence intervals (CIs) were calculated.</p><p><strong>Results: </strong>Sixteen trials met the criteria for inclusion in this review. Four studies were of good quality, 5 were of fair quality, and 7 were of poor quality. Pooled analyses revealed significant reductions in the risks of AAD (RR 0.61, 95% CI 0.47 to 0.79) and CDI (RR 0.37, 95% CI 0.22 to 0.61) among patients randomly assigned to co-administration of probiotics. The number needed to treat for benefit was 11 (95% CI 8 to 20) for AAD and 14 (95% CI 9 to 50) for CDI. With subgroup analysis, significant reductions in rates of both AAD and CDI were retained in the subgroups of good-quality trials, the trials assessing a primarily Lactobacillus-based probiotic formulation, and the trials for which the follow-up period was less than 4 weeks.</p><p><strong>Interpretation: </strong>Probiotics used concurrently with antibiotics reduce the risk of AAD and CDI.</p>","PeriodicalId":88624,"journal":{"name":"Open medicine : a peer-reviewed, independent, open-access journal","volume":"7 2","pages":"e56-67"},"PeriodicalIF":0.0000,"publicationDate":"2013-05-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/94/ba/OpenMed-07-e56.PMC3863752.pdf","citationCount":"0","resultStr":"{\"title\":\"Probiotics for the prevention of antibiotic-associated diarrhea and Clostridium difficile infection among hospitalized patients: systematic review and meta-analysis.\",\"authors\":\"Reena Pattani, Valerie A Palda, Stephen W Hwang, Prakeshkumar S Shah\",\"doi\":\"\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Antibiotic-associated diarrhea (AAD) and Clostridium difficile infection (CDI) are associated with high morbidity, mortality, and health care costs. Probiotics may mitigate the existing disease burden. We performed a systematic review and meta-analysis to evaluate the efficacy of co-administration of probiotics with antibiotics in preventing these adverse outcomes in adult inpatients.</p><p><strong>Methods: </strong>Systematic searches of MEDLINE (1946 to May 2012), Embase (1980 to May 2012), and the Cochrane Central Register of Controlled Trials were undertaken on May 31, 2012, to identify relevant publications. We searched for randomized controlled trials, published in English, of adult inpatients who were receiving antibiotics and who were randomly assigned to co-administration of probiotics or usual care, with or without the use of placebo. Studies were included if they reported on AAD or CDI (or both) as outcomes. Data for predetermined criteria evaluating study characteristics, methods, and risk of bias were extracted. Trials were given a global rating of good, fair, or poor by at least 2 reviewers. Meta-analyses were performed using a random-effects model, and pooled relative risks (RRs) and 95% confidence intervals (CIs) were calculated.</p><p><strong>Results: </strong>Sixteen trials met the criteria for inclusion in this review. Four studies were of good quality, 5 were of fair quality, and 7 were of poor quality. Pooled analyses revealed significant reductions in the risks of AAD (RR 0.61, 95% CI 0.47 to 0.79) and CDI (RR 0.37, 95% CI 0.22 to 0.61) among patients randomly assigned to co-administration of probiotics. The number needed to treat for benefit was 11 (95% CI 8 to 20) for AAD and 14 (95% CI 9 to 50) for CDI. With subgroup analysis, significant reductions in rates of both AAD and CDI were retained in the subgroups of good-quality trials, the trials assessing a primarily Lactobacillus-based probiotic formulation, and the trials for which the follow-up period was less than 4 weeks.</p><p><strong>Interpretation: </strong>Probiotics used concurrently with antibiotics reduce the risk of AAD and CDI.</p>\",\"PeriodicalId\":88624,\"journal\":{\"name\":\"Open medicine : a peer-reviewed, independent, open-access journal\",\"volume\":\"7 2\",\"pages\":\"e56-67\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2013-05-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/94/ba/OpenMed-07-e56.PMC3863752.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Open medicine : a peer-reviewed, independent, open-access journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2013/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open medicine : a peer-reviewed, independent, open-access journal","FirstCategoryId":"1085","ListUrlMain":"","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2013/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景:抗生素相关性腹泻(AAD)和艰难梭菌感染(CDI)与高发病率、高死亡率和高医疗费用相关。益生菌可以减轻现有的疾病负担。我们进行了一项系统回顾和荟萃分析,以评估在成人住院患者中,益生菌与抗生素联合使用对预防这些不良后果的疗效。方法:于2012年5月31日系统检索MEDLINE(1946 - 2012年5月)、Embase(1980 - 2012年5月)和Cochrane Central Register of Controlled Trials,以确定相关文献。我们检索了用英文发表的随机对照试验,这些试验的对象是接受抗生素治疗的成年住院患者,这些患者被随机分配到益生菌或常规治疗组,有或没有使用安慰剂。如果研究结果为AAD或CDI(或两者都有),则纳入研究。提取用于评估研究特征、方法和偏倚风险的预定标准的数据。试验由至少2位审稿人给予良好、一般或较差的全球评级。采用随机效应模型进行meta分析,计算合并相对危险度(rr)和95%置信区间(ci)。结果:16项试验符合纳入本综述的标准。4项研究质量良好,5项研究质量一般,7项研究质量较差。综合分析显示,在随机分配给益生菌的患者中,AAD (RR 0.61, 95% CI 0.47至0.79)和CDI (RR 0.37, 95% CI 0.22至0.61)的风险显著降低。对于AAD,需要治疗的人数为11人(95% CI为8 ~ 20),对于CDI,需要治疗的人数为14人(95% CI为9 ~ 50)。通过亚组分析,在高质量试验的亚组中,主要评估以乳酸杆菌为基础的益生菌制剂的试验,以及随访时间少于4周的试验中,AAD和CDI的发生率均有显著降低。解释:益生菌与抗生素同时使用可降低AAD和CDI的风险。
Probiotics for the prevention of antibiotic-associated diarrhea and Clostridium difficile infection among hospitalized patients: systematic review and meta-analysis.
Background: Antibiotic-associated diarrhea (AAD) and Clostridium difficile infection (CDI) are associated with high morbidity, mortality, and health care costs. Probiotics may mitigate the existing disease burden. We performed a systematic review and meta-analysis to evaluate the efficacy of co-administration of probiotics with antibiotics in preventing these adverse outcomes in adult inpatients.
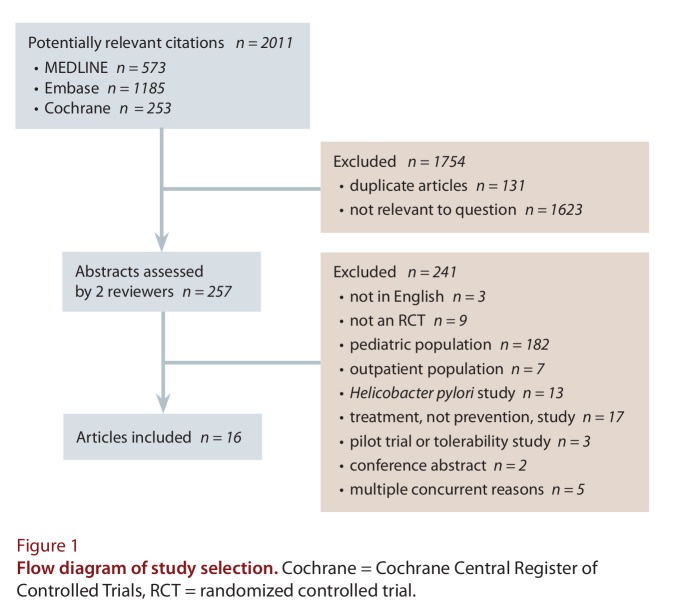
Methods: Systematic searches of MEDLINE (1946 to May 2012), Embase (1980 to May 2012), and the Cochrane Central Register of Controlled Trials were undertaken on May 31, 2012, to identify relevant publications. We searched for randomized controlled trials, published in English, of adult inpatients who were receiving antibiotics and who were randomly assigned to co-administration of probiotics or usual care, with or without the use of placebo. Studies were included if they reported on AAD or CDI (or both) as outcomes. Data for predetermined criteria evaluating study characteristics, methods, and risk of bias were extracted. Trials were given a global rating of good, fair, or poor by at least 2 reviewers. Meta-analyses were performed using a random-effects model, and pooled relative risks (RRs) and 95% confidence intervals (CIs) were calculated.
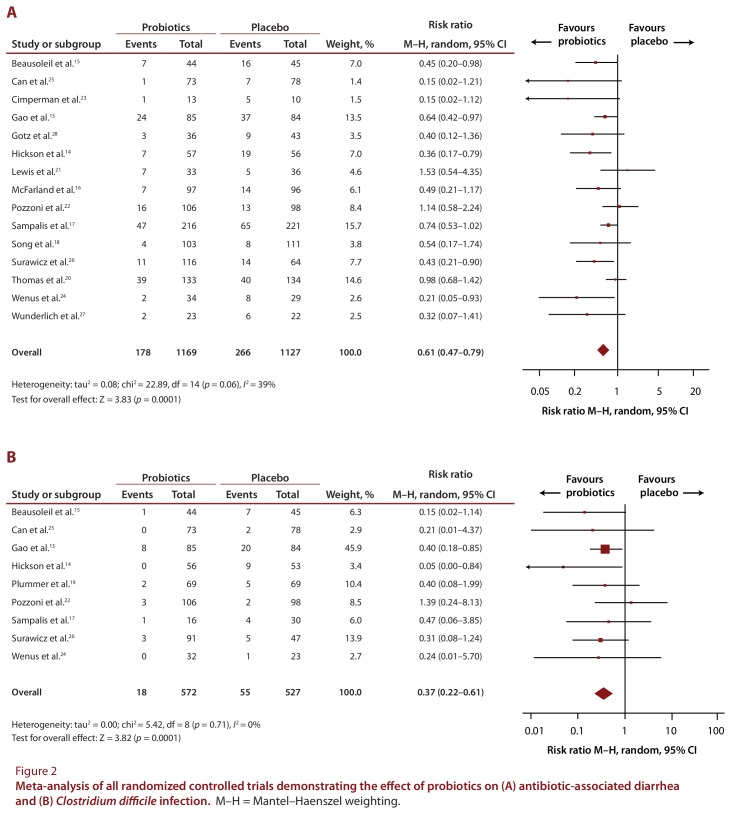
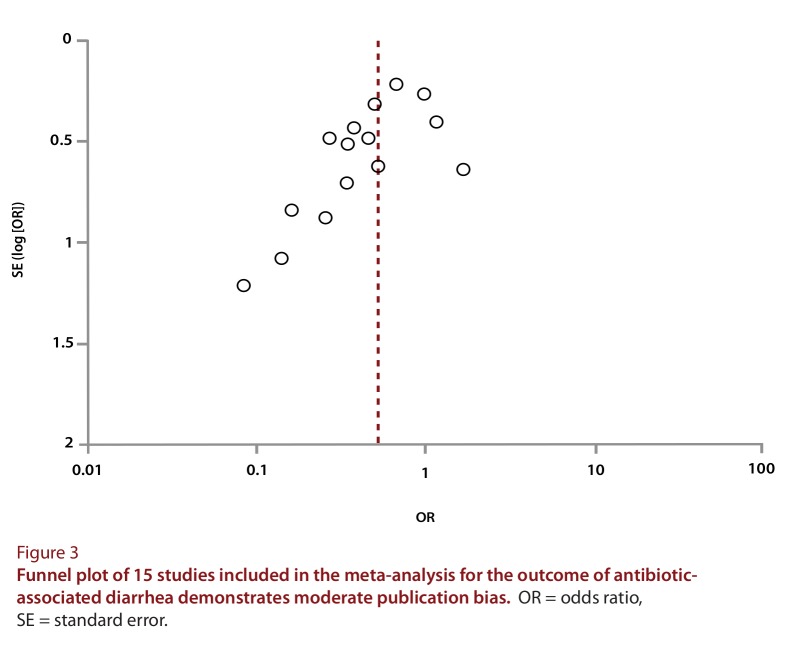
Results: Sixteen trials met the criteria for inclusion in this review. Four studies were of good quality, 5 were of fair quality, and 7 were of poor quality. Pooled analyses revealed significant reductions in the risks of AAD (RR 0.61, 95% CI 0.47 to 0.79) and CDI (RR 0.37, 95% CI 0.22 to 0.61) among patients randomly assigned to co-administration of probiotics. The number needed to treat for benefit was 11 (95% CI 8 to 20) for AAD and 14 (95% CI 9 to 50) for CDI. With subgroup analysis, significant reductions in rates of both AAD and CDI were retained in the subgroups of good-quality trials, the trials assessing a primarily Lactobacillus-based probiotic formulation, and the trials for which the follow-up period was less than 4 weeks.
Interpretation: Probiotics used concurrently with antibiotics reduce the risk of AAD and CDI.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


